Chapter 19 Treatment Plans for Partially and Completely Edentulous Arches in Implant Dentistry
PARTIALLY EDENTULOUS ARCHES
To organize treatment plans in a consistent approach, a classification of patient conditions is necessary. Because more than 65,000 possible combinations of teeth and edentulous spaces exist in a single arch, no universal agreement exists regarding the use of any one classification system. Numerous classifications have been proposed for partially edentulous arches. Their use allows the profession to visualize and communicate the relationship of hard and soft structures. This chapter reviews a classification for diagnosis and treatment planning for patients who are partially or completely edentulous and require implant prostheses. By using this classification, which the author first presented in 1985, the doctor is able to convey the dimensions of the bone available in the edentulous area and also indicate the strategic position of the segment to be restored.15
HISTORY
Cummer,1 Kennedy,2 and Bailyn3 originally proposed the classifications of partially edentulous arches that are most familiar to the profession. These classifications were developed to organize removable partial denture (RPD) designs and concepts. Other classifications have also been proposed4–14 (including one by the American College of Prosthodontists), none of which has been universally accepted. The Kennedy classification, however, has been taught in most American dental schools.
The Kennedy classification divides partially edentulous arches into four classes.2 Class I has bilateral posterior edentulous spaces, Class II has a unilateral posterior edentulous space, Class III has an intradental edentulous area, and Class IV has an anterior edentulous area that crosses the midline.
The Kennedy classification is difficult to use in many situations without certain qualifying rules. The eight Applegate rules are used to help clarify the system.11 They may be summarized in three general principles. The first principle is that the classification should include only natural teeth involved in the final prosthesis and follow rather than precede any extractions of teeth that might alter the original classification. This concept, for example, considers whether second or third molars are to be replaced in the final restoration. The second rule is that the most posterior edentulous area always determines the classification. The third principle is that edentulous areas, other than those determining the classification, are referred to as modifications and are designated only by their number. The extent of the modification is not considered.
CLASSIFICATION OF PARTIALLY EDENTULOUS ARCHES
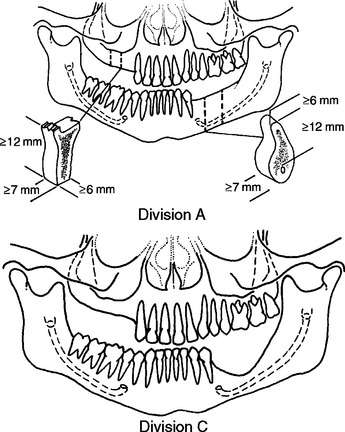
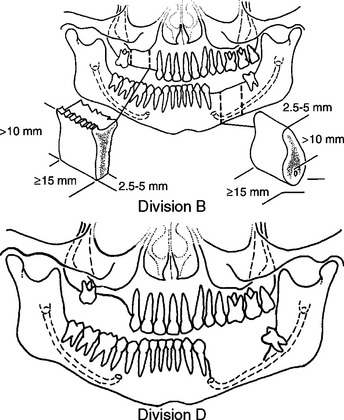
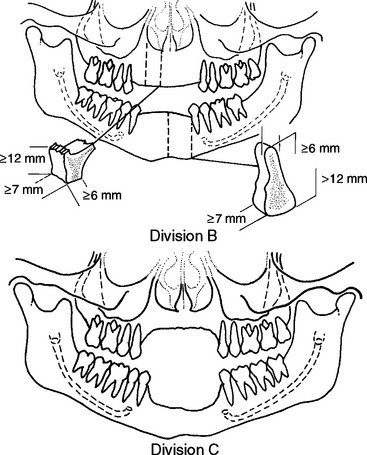
The implant dentistry bone volume classification developed by Misch and Judy in 1985 may be used to build on the four classes of partial edentulism described in the Kennedy-Applegate system.15,16 This facilitates communication of teeth positions and the primary edentulous sites among the large segment of practitioners already familiar with this classification, and it enables the use of common treatment methods and principles established for each class. The implant dentistry classification for partially edentulous patients by Misch and Judy also includes the same four available bone volume divisions previously presented for edentulous areas. Other intradental edentulous regions that are not responsible for the Kennedy-Applegate class determination are not specified within the available bone section, should implants not be considered in the modification region. However, if the modification segment is also included in the treatment plan, then it is listed, followed by the available bone division it characterizes (Box 19-1).
Box 19-1 Implant Dentistry Classification of Partially Edentulous Arches
Class I: Partially Edentulous Arch with Bilateral Edentulous Areas Posterior to Remaining Natural Teeth
Division A
Division B
Division C
Treatment Planning: Class I
In Class I patients, distal edentulous segments are bilateral and natural anterior teeth are present. The majority of these arches are only missing molars, and almost all have retained at least the anterior incisors and canines.17 Therefore, once restored to proper occlusal vertical dimension, the natural anterior teeth contribute to the distribution of forces throughout the mouth in centric relation occlusion. More importantly, when opposing natural teeth or in fixed implant prosthesis, they also permit excursions during mandibular movement to disclude the posterior implant-supported prostheses and protect them from lateral forces. However, many of these mandibular Class I patients oppose a maxillary denture, in which case bilateral balance is more appropriate.
The Class I patient is more likely to wear a RPD than Class II or III patients because mastication and/or support of an opposing removable prosthesis is more difficult when not wearing a mandibular prosthesis. The posterior soft tissue–supported Class I partial dentures are designed to either primary load the edentulous regions or the natural anterior teeth. The clasp design, which places less force on the tooth (e.g., bar clasp including t, y rpi), will place more force on the bone. The RPDs, which place more force on the abutment teeth (e.g., precision partial dentures), will place less force on the bone. In either case, the removable prosthesis often accelerates the posterior bone loss. In addition, a partial denture that is not well designed or maintained distributes additional loads to abutment teeth and may even contribute to poor periodontal health. The combinations of these conditions lead to bone loss in the edentulous regions and poorer adjacent natural abutments.18–20 As a result, it is this author’s observation that long-term Class I patients who have been wearing an RPD often exhibit Division C ridges and mobile abutment teeth.
Division B Treatment Plans
The patient missing molars and both premolars requires additional implant support. Four Division B root forms may be the foundation of an independent fixed partial denture (FPD) in the mandible, depending on the other stress factors. If stress factors are too great (as a result of parafunction) or bone density is poor (as in the maxilla), then the Division B bone should be augmented to Division A before larger-diameter implant insertion. The anterior teeth in Class I patients should provide disclusion of the posterior implants during all excursions when opposing natural teeth or a fixed prosthesis. Molar endosteal implants should not be rigidly cross-splinted to each other in the Class I patient. Flexure of the mandible during opening may cause a rigid splint to exert lateral forces on the posterior implants. Therefore independent restorations are indicated.
Division C Treatment Plans
In the mandible, the third option for the Class I, Division C patient is to place unilateral subperiosteal implants or disc implants above the canal (Figure 19-1). The disc implants support independent posterior fixed prostheses bilaterally.
The fourth treatment option in the mandible is nerve repositioning and endosteal implants in Class I patients who are poor candidates for bone augmentation or subperiosteal implants. Risks of long-term paresthesia exist that may include hyperesthesia and pain. Reports in the literature concern dysesthesia and fracture of the severely atrophic mandible.21,22 In addition, the gain of height in the C–h mandible may only permit the placement of implants 10 mm high, still insufficient to compensate for the increased crown height and resultant unfavorable crown/implant ratio.
Treatment Planning: Class II
Kennedy-Applegate Class II partially edentulous patients are missing teeth in one posterior segment (see Box 19-1). These patients are often able to function without a removable restoration and are less likely to tolerate or overcome the minor complications of wearing the prosthesis. As a result, they are not as likely to wear a removable restoration. The available bone is therefore often adequate for endosteal implants, even when long-term edentulism has been present. However, the local bone density may be decreased. Endosteal implants with minimum osteoplasty are a common modality in these patients, who are more often Class II, Division A or B types.23,24
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


