Chapter 14 The Edentulous Mandible: An Organized Approach to Implant-Supported Overdentures
The dental profession and the public are more aware of the problems associated with a complete mandibular denture than any other dental prosthesis. The placement of implants enhances the support, retention, and stability of an overdenture. As a result, patients are very willing to accept a treatment plan for a mandibular implant overdenture. There is greater flexibility in implant position or prosthesis fabrication with a mandibular implant overdenture, and, as a result, it is also an ideal treatment modality to begin a learning curve in implant dentistry. Therefore one of the most beneficial treatments rendered to patients is also one of the best introductions for a dentist into the discipline of implant dentistry. In comparison, maxillary implants for overdentures are not used as often and are also more difficult to place and restore.
The concept of mandibular implant–supported overdentures has been used for many years. Successful reports were published originally with mandibular subperiostal implants or with immediately loaded and stabilized root form implants in the anterior mandible.1,2 An increased awareness from the profession and patients allows a variety of clinical situations, bone densities, biomechanics, and patients’ desires to restore an ever-growing number of patients with implant-supported overdentures.3–32 As the data gathered on this prosthetic modality grow, overdentures are gaining even greater acceptance and justifying their place in the armamentarium of the implant dentist.
Because of the long hiatus between dental visits, the amount of resorption from initial denture delivery to the next professional interaction already has caused the destruction of the original alveolar process. The bone loss that occurs during the first year after tooth loss is 10 times greater than in following years. In the case of multiple extractions, this often means a 4-mm vertical bone loss within the first 6 months. As the bony ridge resorbs, the muscle attachments become level with the edentulous ridge.33–35
The next progression in the implant philosophy is to convert all mandibular implant and soft tissue–supported restorations to a completely implant-supported prosthesis. The majority of mandibular overdentures are supported by two implants anterior to the foraminae and soft tissue support in the posterior regions (Figure 14-1). Yet posterior bone loss occurs four times faster than anterior bone loss. In the completely edentulous patient, the eventual paresthesia and mandibular body fractures are primarily from posterior bone loss. The anterior implants allow improved anterior bone maintenance, and the prosthesis benefits from improved function, retention, and stability. However, the lack of posterior support in two- and three-implant overdentures may cause accelerated posterior bone loss. To the contrary, studies by Wright et al.30 and Reddy et al.36 found prostheses completely supported by implants in the edentulous mandible actually may increase the posterior bone volume (even though posterior implants are not inserted). As a result, complete implant-supported restorations should be the restoration of choice.
Financial considerations have been identified as the reason for the selection of a limited treatment, which may consist of two or three implants to support the overdenture.37–39 These restorations may be used as transitional devices until the patient can afford to upgrade the restoration. When a partially edentulous patient cannot afford to replace four missing first molars, the dentist often will replace one at a time over many years. Likewise, the dental implant team can insert one or two additional implants every few years until finally a complete implant-supported prosthesis is delivered.
REVIEW OF THE LITERATURE
In 1986 a multicenter study reported on 1739 implants placed in the mandibular symphysis of 484 patients. The implants were loaded immediately and restored with bars and overdentures with clips as retention. The overall success rate was 94.2 Engquist et al.3 reported a 6% to 7% implant failure for mandibular implant–supported overdentures and a 19% to 35% failure for maxillary implant overdentures. Hyperplasia below the bar occurred in 25% of the patients. Prosthetic complications were not reported. Jemt et al.4 reported on a 5-year prospective, multicenter study on 30 maxillae (117 Brånemark implants) and 103 mandibles with 393 implants. Survival rates in the mandible were 94.5% for implants and 100% for prostheses; in the maxilla, the survival rates were 72.4% for implants and 77.9% for prostheses. Higher failure rates in the maxilla were related directly to poor density and quantity of bone with a characteristic cluster failure pattern.
Wismeijer et al.5 reported on 64 patients with 218 titanium plasma-sprayed implants, with a 97% survival with overdentures in a 6.5-year evaluation. Naert et al.14 found 100% implant success at 5 years for overdentures with different anchorage systems. In Belgium, Naert at al. reported on 207 consecutively treated patients with 449 Brånemark implants and Dolder-bar overdentures. In this report, the cumulative implant failure rate was 3% at the 10-year benchmark.9,10 In this long-term report, prosthetic complications related to overdenture relining and loose retention occurred 10% of the time. More care was needed if ball attachments were used rather than a Dolder bar.9 In a 10-year study reporting on attachment methods, balls provided the greatest retention and magnets always scored the lowest.10 Similarly, Hutton et al.11 reported 97% survival rates for mandibular overdentures.
Misch12 reported less than 1% implant failure and no prosthesis failure over a 7-year period with 147 patients when using the organized treatment options and prosthetic guidelines presented in this chapter. Kline et al.13 reported on 266 implant-supported overdentures for 51 patients, with an implant survival rate of 99.6% and a prosthesis survival rate of 100%. Mericke-Stern et al.16 reported 95% implant survival with two implant overdentures. In a randomized clinical report, Awad et al.6 compared satisfaction and function in complete dentures (48 patients) versus two implant-supported overdentures (IODs) in 56 patients. There was significantly higher satisfaction, comfort, and chewing ability in the IOD group. A similar study in a senior population yielded similar results.7 Thomason et al.,8 in the United Kingdom, reported a 36% higher satisfaction for the implant IOD patients than the complete denture wearers in the criteria of comfort, stability, and chewing. In Canada, Attard and Zarb40 followed IOD wearers for 20 years with a success rate of 84% and 87% for prosthesis and implants, respectively. In a 10-year study of IODs in Israel, with 285 implants and 69 implant over dentures, Schwartz-Arad et al. reported implant survival was 96.1% with higher success rates in the mandible.41 Many reports have been published over the last two decades that conclude that implant-supported overdentures represent a valid beneficial option for denture wearers.3–41 It should be noted that the majority of reports are for implant overdentures supported by only two implants.
ADVANTAGES OF IMPLANT OVERDENTURES
The patient gains several advantages with an implant-supported prosthesis (Box 14-1). Minimal bone resorption of the anterior residual ridge occurs with the placement of implants. After the extraction of mandibular teeth, an average of 4-mm vertical bone loss occurs during the first year after treatment. This bone loss continues over the next 25 years, with the mandible experiencing a fourfold greater vertical bone loss than the maxilla.35 The bone under an overdenture may resorb as little as 0.6 mm vertically over 5 years, and long-term resorption may remain at less than 0.05 mm per year.4,40,42,43
Soft tissue abrasions and accelerated bone loss are more symptomatic of horizontal movement of the prosthesis under lateral forces. An implant-supported overdenture may limit lateral movements and direct more longitudinal forces. A mandibular denture may move 10 mm during function. Under these conditions, specific occlusal contacts and the control of masticatory forces are nearly impossible. An implant overdenture provides stability of the prosthesis, and the patient is able consistently to reproduce a determined centric occlusion.44
A study of chewing efficiency compared wearers of complete dentures with wearers of implant-supported overdentures. The complete denture group needed 1.5 to 3.6 times the number of chewing strokes compared with the overdenture group.45 The chewing efficiency with an implant overdenture is improved by 20% compared with a traditional complete denture.6,7,46,47
Higher bite forces have been documented for mandibular overdentures on implants. The maximum occlusal force of a patient with dentures may improve 300% with an implant-supported prosthesis.48 Mericke-Stern49 and Mericke-Stern et al.50 compared mastication between root overdentures and implant overdentures. The former was more discriminative, whereas the latter developed slightly harder chewing strokes and tended to masticate more vertically. Jemt et al.51 showed a decrease in occlusal force when the bar connecting implants was removed, which they attributed to the loss of support, stability, and retention. If enough implant support is provided, the resulting prosthesis may be completely supported, retained, and stabilized by the implant (removable prosthesis type 4 [RP-4]).
The complete mandibular denture often moves during mandibular jaw movements during function and speech. The contraction of the mentalis, buccinator, or mylohyoid muscles may lift the denture off the soft tissue. As a consequence, the teeth may touch during speech and elicit clicking noises. The retentive implant overdenture remains in place during mandibular movement. The tongue and perioral musculature may resume a more normal position because they are not required to limit mandibular denture movement.
Soft and hard tissue defects from tumor excision or trauma do not permit the successful rehabilitation of the patient with traditional denture support. Hemimandibulectomy patients and other maxillofacial patients also may be restored successfully with an implant overdenture.52,53
The implant overdenture also provides many practical advantages over the implant-supported complete fixed partial denture (Box 14-2). Fewer implants are required, because soft tissue areas may provide additional support. Regions of inadequate bone for implant placement therefore may be eliminated from the treatment plan, rather than necessitating bone grafts or placing implants with poorer prognosis. Abutments do not require a specific mesiodistal placement because the prosthesis completely covers the implant abutments.
Box 14-2 Implant Overdenture Advantages versus Fixed Prosthesis
An overdenture may be removed at bedtime to reduce the noxious effect of nocturnal parafunction, which increases stresses on the implant support system. The overdenture may provide stress relief between the superstructure and prosthesis, and the soft tissue may share a portion of the occlusal load. The prosthesis is usually easier to repair than a fixed restoration. Reduced laboratory fees and fewer implants allow the restoration of patients at reduced costs compared with a fixed prosthesis. In addition, long-term denture patients do not appear to have a psychologic problem associated with the ability to remove their implant prostheses.54–62
When cost is a factor, two implant-retained IODs may improve the patient’s condition at a lower overall treatment cost than a fixed implant–supported prosthesis.42,44,63 A survey by Carlsson et al.64 in 10 countries indicated a wide range of treatment options. The proportion of implant overdentures selection versus fixed implant dentures was highest in the Netherlands (93%) and lowest in Sweden and Greece (12%). Cost was cited as the number one determining factor in the choice.
DISADVANTAGES OF IMPLANT OVERDENTURES
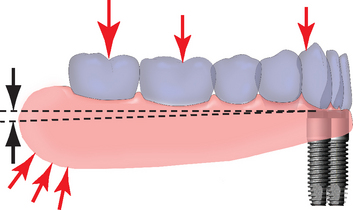
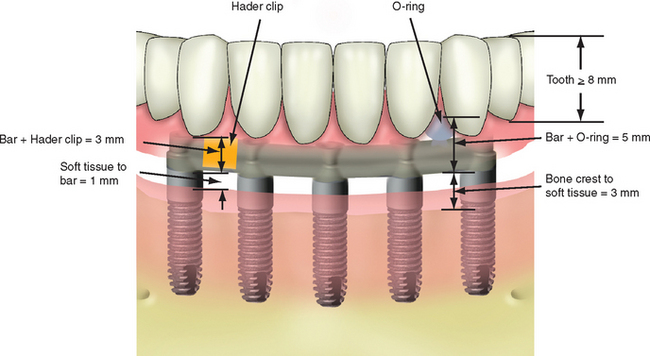
The mandibular overdenture treatment plan requires more than 12 mm of space between crestal bone and the occlusal plane (Figure 14-2). When sufficient crown height space is lacking and the prosthesis is more prone to component fatigue and fracture, an overdenture is more difficult to fabricate than a porcelain-to-metal fixed prosthesis. The 12-mm minimum crown height space provides adequate bulk of acrylic to resist fracture, space to set denture teeth without modification, and room for attachments, bars, soft tissue, and hygiene. In the mandible, the soft tissue is often 1 to 3 mm thick above the bone, so the occlusal plane to soft tissue should be at least 9 to 11 mm in height. An osteoplasty to increase crown height space before implant placement or a fixed restoration is often indicated when abundant bone height and width are present.
Mandibular overdenture wearers often incur greater long-term expenses than those with fixed restorations. Attachments such as O-rings or clips wear and must be replaced regularly. Replacements appear more frequent during the first year, but remain a necessary maintenance step.17,20,34,65–72 Denture teeth wear faster on an implant overdenture than with a traditional denture because bite force and masticatory dynamics are improved. A new overdenture often is required at 5- to 7-year increments because of denture tooth wear and soft tissue support changes. Therefore patient education of the long-term maintenance requirement should be outlined at the onset of implant therapy.73
A primary concern for RP-5 overdentures compared with RP-4 or fixed restorations is the continued bone loss in the posterior regions. The posterior bone resorbs faster than the anterior bone, and implant prostheses with posterior soft tissue support may accelerate posterior bone resorption two to three times faster than in a complete denture wearer.73–75 By contrast, patients wearing fixed implant–supported prostheses showed no bone loss and usual occurrences of bone apposition.76,77 Therefore the short-term benefit of decreased cost may be offset by the accelerated bone loss that is a primary consideration, especially in the younger edentulous patient. As previously discussed, all implant overdentures would benefit if they were completely implant supported, and the recommendation is to consider a RP-5 prosthesis as an interim device designed to enhance the function of the patient. These prostheses should not be considered as an end result for all patients. Instead, a regular evaluation of patients’ performance paired with patient education should enable the transformation to a RP-4 restoration. In addition, reports indicate that mandibular implant overdentures may cause a combination-like syndrome, with increased looseness, subjective loss of fit, and midline fracture of the upper denture.78–82 Although not yet established as a cause-and-effect situation, the condition also appears to be controlled by the choice of proper occlusal scheme.80
A side effect of a mandibular overdenture is food impaction. The flanges of the prosthesis do not extend to the floor of the mouth in the rest position (to eliminate sore spots caused by elevation of the floor of the mouth during swallowing). However, during eating, food particles migrate and become impacted under the prosthesis during swallowing. A similar condition is found with a traditional denture. However, because a lower denture “floats” during function, the food more readily goes under and out, whereas the implant overdenture traps the food debris against the implants, bars, and attachments (Box 14-3).
OVERDENTURE MOVEMENT
Classification of Prosthesis Movement
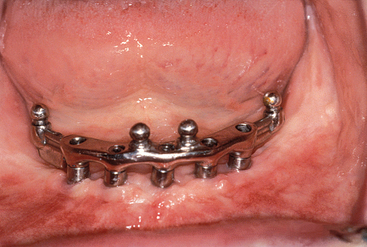
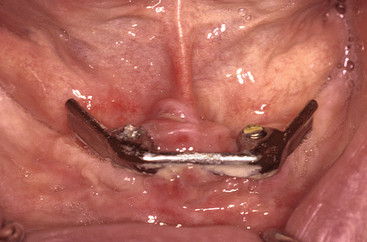
The dentist evaluates the prosthesis movement when seating the restoration. If the prosthesis is rigid when in place but can be removed, the prosthesis movement is labeled PM-0, regardless of the attachments used. For example, O-rings may provide motion in six different directions. But if four O-rings are placed along a complete arch bar, and the prosthesis rests on the bar, the situation may result in a PM-0 restoration (Figure 14-3). A hingelike prosthesis movement permits movement in two planes (PM-2) and most often uses a hingelike attachment. For example, the Dolder bar and clip without a spacer or Hader bar and clip are the most commonly used hingelike attachment. A Dolder bar is egg shaped in cross section, and a Hader bar is round. A clip attachment may rotate directly on the Dolder bar. A Hader bar is more flexible because round bars flex to the power of 4 related to the distance and other bar shapes flex to the power of 3. As a result, an apron often is added to the tissue side of the Hader bar to limit metal flexure, which might contribute to unretained abutments or bar fracture. It should be noted that for these systems to function efficiently, the hinge attachment needs to be perpendicular to the axis of prosthesis rotation, so the prosthesis movement also will be in two planes (i.e., PM-2). If the Hader or Dolder bar is at an angle or parallel to the direction of desired rotation, the prosthesis is more rigid and may resemble a PM-0 system (Figure 14-4).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


