Chapter 11
Functional appliances
THE PROBLEM
These appliances are mainly used when correction is needed in Class II malocclusions. Their aim is to encourage forward development of the mandible which can reduce a significantly increased overjet (horizontal distance between the upper and lower incisor teeth) and correct a Class II molar relation to Class I.
When a patient comes into the surgery concerned that their upper teeth appear to ‘stick out’, they may also have:
- an underdeveloped mandible (and also a receding chin)
- a lower lip that curls under the upper teeth, often becoming trapped behind them
This makes the upper incisors seem to protrude even further.
A clinical assessment often shows that the front teeth are not positioned too far forward in relation to the upper face.
The problem is that the lower jaw has not grown sufficiently and is shorter than the upper.
The clinician may therefore decide that functional appliance therapy is needed.
They are designed to harness the power of the jaw and facial muscles to correct the occlusal relationship between the upper and lower arches. They hold the ‘postured’ mandible forward and are most effective in a growing patient.
They can therefore be used in the later mixed dentition through puberty to about 14 years of age.
In very severe cases of jaw-length discrepancy, particularly in older patients, orthognathic treatment (an osteotomy) is a treatment option.
For less severe cases and when the patient is still growing, functional appliance therapy is often the treatment of choice.
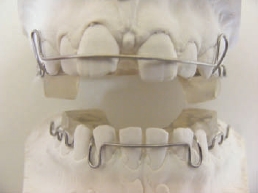
Most functional appliances (Figure 11.1) are removable and can be taken in and out for eating and cleaning.
Figure 11.1 Functional appliance.

However, the success of these appliances is related to the compliance of the patient in wearing them as advised.
Patients who wear them intermittently make slow progress and, if treatment is not completed, can find that this can quickly relapse.
THE SOLUTION
The functional appliance works by movement of the teeth and alveolar bone with some forward mandibular development too.
They rely on oro-facial muscles to supply the force which, transmitted through the functional appliance, produces intermaxillary traction.
Before the appliance is fitted, the overjet is measured and recorded and this is done again at the end of treatment.
When the treatment is completed, it should be possible to gradually remove the appliance and find that the mandible and occlusion remain stable.
TYPES OF FUNCTIONAL APPLIANCE
There are many types of functional appliance. Because there seems to be no accepted classification of functional appliances many are known by the name of the clinician who developed them.
For example
the Andresen activator:
- is a tooth-borne appliance
- is basically an upper and lower appliance fused together, where the lower one is advanced forward of the upper
- is made of acrylic and wire
- is successful on Class II/I cases with well-aligned arches
Figure 11.2 Clark Twin Block front view.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


