Force Factors Related to Patient Conditions (A Determinant for Implant Number and Size)
Carl E. Misch
Biomechanical stress is a significant risk factor in implant dentistry. Its magnitude is directly related to force. As a result, an increase in any dental force factor magnifies the risk of stress-related complications. Mechanical complication rates for implant prostheses are often the highest of all complications reported in the literature.1 Mechanical complications include prosthetic and abutment screw loosening and may range to 8% for single teeth, 6% for multiple implants, and 3% for overdentures. Uncemented restorations also occur in more than 10% of the restorations. Porcelain fracture may affect up to half the patients with high stress factors, and resin veneer implant fixed partial dentures fracture 20% of the time. Crestal bone loss may be related to occlusal excessive forces.2 Implant failure may also occur from overload and result in prosthesis failure. Retentive clips or attachments fracture in overdentures; the risk factor may average one in five. The fracture of the opposing prosthesis also increases in direct relationship to the force, with an average of 12% in implant overdentures opposing a denture. Fracture of the framework or substructure may also occur as a result of an increase in biomechanical forces.3 In addition, implant body fracture may result from fatigue loading of the implant but fortunately occurs less often than most complications. All of these mechanical complications are often caused by excessive stress or cycles applied to the implant–prosthetic system (Box 10-1). Hence, force factors are an important aspect to consider when developing a treatment plan for implant dentistry.
The greater the biomechanical force, the fewer the number of cycles before fracture, so the incidence increases as the force increases. Different patient conditions place different amounts of force in magnitude, duration, type, and direction. In addition, several factors may multiply the number of loading cycles or increase the effect of these other conditions.
After the prosthesis option and key implant positions are determined, the potential force levels that will be exerted on the prosthesis should be evaluated and accounted for in order to modify the overall treatment plan. Several elements observed during the dental evaluation predict additional forces on future implant abutments. The initial implant healing, loading survival, marginal crestal bone loss, incidence of abutment or prosthetic screw loosening, unretained restorations, occlusal material fracture, and component fracture are all influenced by the patient’s occlusal force factors. In addition, the patient force factors are a major influence on implant number and ideal size. There are five primary patient force factors affecting the stress environment of the implant and prosthesis: parafunction, crown height space (CHS), masticatory dynamics, arch position, and nature of the opposing dentition (Box 10-2).
Normal Forces Exerted on Teeth
The greatest natural forces exerted against teeth, and thus against implants, occur during mastication.4,5 These forces are primarily perpendicular to the occlusal plane in the posterior regions, are of short duration, occur only during brief periods of the day, and range from 5 to 44 lb for natural teeth. The actual force on each tooth during function has been recorded on strain gauges in inlays.6 A force of 28 psi was observed during chewing a raw carrot, and 21 psi was observed to chew meat. The actual time during which chewing forces are applied on the teeth is about 9 minutes each day.7 The perioral musculature and tongue exert a more constant yet lighter horizontal force on the teeth or on implants. These forces reach 3 to 5 psi during swallowing.8 A person swallows 25 times per hour while awake and 10 times per hour while sleeping, for a total of 480 times each day.7 Therefore, natural forces against teeth are primarily in their long axis, less than 30 psi, and for less than 30 minutes per day for all normal forces of deglutition and mastication (Box 10-3).
The maximum bite force differs from mastication force, varies widely among individuals, and depends on the state of the dentition and masticatory musculature.9 There have been many attempts to quantify the normal maximum bite force. In 1681, Borelli suspended weights on a thread over the molars while the mandible was open. The maximum load recorded for which the person was still able to close ranged from 132 to 440 lb. A force of 165 lb was recorded on a gnathodynamometer, the first instrument to record occlusal force, which was developed by Patrick and Dennis in 1892. Black improved this early design and recorded average forces of approximately 170 lb.10 The forces on the chewing side and the opposite side appear very similar in amplitude11 (Table 10-1). More recent studies indicate normal maximum vertical biting forces on teeth can range from 45 to 550 psi.12,13
TABLE 10-1
Mean Maximum Biting Force Recorded on Natural Teeth or Implants*
| Authors (Year) | Natural Teeth or Dental Implants | Mean Maximum Masticatory Force |
| Carr and Laney79 (1987) | Conventional denture | 59 N |
| Implant-supported prostheses | 112.9 N | |
| Morneburg and Proschel21 (2002) | Implant-supported three-unit FPD | 220 N |
| Single implant: anterior | 91 N | |
| Single implant: posterior | 12 N | |
| Fontijn-Tekamp et al.87 (1998) | Implant-supported prostheses | (unilateral) |
| Molar region | 50–400 N | |
| Incisal region | 25–170 N | |
| Mericske-Stern and Zarb90 (1996) | Complete denture/implant-supported prostheses | 35–330 N |
| van Eijden12 (1991) | Canine | 469 ± 85 N |
| Second premolar | 583 ± 99 N | |
| Second molar | 723 ± 138 N | |
| Braun et al.13 (1995) | Natural teeth | 738 ± 209 N (male > female) |
| Raadsheer et al.78 (1999) | Male teeth | 545.7 N |
| Female teeth | 383.6 N |
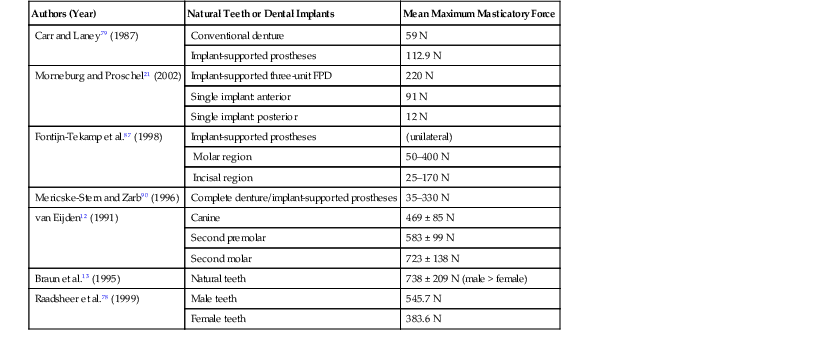
* Comparison of available studies examining masticatory forces generated under varying loading condition. Study results are reported in Newtons (N) of force unless otherwise indicated. Differences between male and female force generation are noted in applicable studies.
FPD, Fixed partial dentures.
Forces of mastication placed on implant-supported bridges have been measured up to four times greater than natural teeth.14 Implant-supported prostheses have less occlusal awareness than natural teeth, so the opposing implant prostheses do not reduce velocity before contact as with the natural dentition. Hence, the patient force factors are even more important to evaluate for implant prostheses.15–21
It should be emphasized that the maximum bite forces are not expressed by our patients in any routine fashion. However, there are conditions that approach these values and increase our risks of occlusal overload on the implant prosthesis. Most noteworthy are the parafunctional forces of bruxism and clenching because they modify the amount of force and the duration of force.
Parafunction
Parafunctional forces on teeth or implants are characterized by repeated or sustained occlusion and have long been recognized as harmful to the stomatognathic system.22 These forces are also damaging when applied to implant prostheses.23,24 The lack of rigid fixation during implant healing may be a result of parafunction on soft tissue–borne prostheses overlying the submerged implant. The most common cause of both early and late implant failure after successful surgical fixation is the result of parafunction. Such complications occur with greater frequency in the maxilla because of a decrease in bone density and an increase in the moment of force.25 The presence of these parafunctional conditions must be carefully noted during the early phases of treatment planning.
Nadler has classified the causes of parafunction or nonfunctional tooth contact into the following six categories26:
Local factors include tooth form or occlusion, as well as soft tissue changes such as ulcerations or pericoronitis. Systemic factors include cerebral palsy, epilepsy, and drug-related dyskinesia. Psychological causes occur with the greatest frequency and include the release of emotional tension or anxiety.27 Occupational factors concern professionals such as dentists, athletes, and precision workers, as well as seamstresses and musicians who develop altered oral habits. Involuntary movements that provoke bracing of the jaws, such as during lifting of heavy objects or sudden stops while driving, contribute to parafunction. Voluntary causes include chewing gum or pencils, bracing a telephone between the head and shoulder, and pipe smoking.
The parafunctional groups presented in this chapter are divided into bruxism, clenching, and tongue thrust or size. The dental literature usually does not identify bruxism and clenching as separate entities. Although several aspects of treatment are similar, their diagnosis and treatment are in some ways different. As such, they are presented as different entities in this discussion.
The magnitude of parafunction may be categorized as absent, mild, moderate, or severe.23 Bruxism and clenching are the most critical factors to evaluate in any implant reconstruction. No long-term success will be obtained with severe parafunction of bruxism or clenching. Therefore, the dentist should always try to diagnose the presence of these two conditions.
This does not mean that patients with moderate and severe parafunction cannot be treated with implants. A physician treats a patient with uncontrolled diabetes; however, the patient may lose their vision or need his or her feet amputated despite treatment. Unsuccessful treatment of the person with diabetes may not be the fault of the physician. Not recognizing diabetes in the presence of obvious signs and symptoms, of course, is another issue. Because patients with moderate to severe parafunction represent so many additional risks in implant dentistry, one must be aware of these conditions and the methods to reduce their noxious effects on the entire implant-related system. Unfortunately, parafunction may be a difficult entity to diagnose, especially if the patient is completely edentulous and is wearing a recently fabricated prosthesis.
Bruxism
Bruxism primarily concerns the horizontal, nonfunctional grinding of teeth. The forces involved are in significant excess of normal physiologic masticatory loads. Bruxism may affect the teeth, muscles, joints, bone, implants, and prostheses.28 These forces may occur while the patient is awake or asleep and may generate increased force on the system several hours per day. Bruxism is the most common oral habit. Sleep clinic studies have evaluated nocturnal bruxism and found approximately 10% of those observed had obvious movement of the mandible with occlusal contacts.29,30 More than half of these patients had tooth wear affecting esthetics. Only 8% of these patients were aware of their nocturnal bruxism, and only 25% of the patients’ spouses were aware of the nocturnal habit. Muscle tenderness in the morning was observed less than 10% of the time.31 A study on bruxing patients with implants showed 80% of sleep bruxism occurred during light sleep stages but did not cause arousal.32 Therefore, patients with bruxism may or may not have obvious tooth wear affecting esthetics; may brux nocturnally, but their bed partners do not know most of the time; rarely have muscle tenderness when they are awake; and are usually unaware of their oral habit. In other words, nocturnal bruxism is sometimes difficult to diagnose.33
The maximum biting force of bruxing patients is greater than average. Just as an experienced weightlifter can lift more weight, the patient constantly exercising the muscles of mastication develops a greater bite force. A man who chews paraffin wax for an hour each day for a month can increase the bite force from 118 to 140 psi within 1 week.34 Chewing gum, bruxism, and clenching may accomplish the same feat. Eskimos, with a very tenacious diet and who chew their leather to soften it before fabrication of clothing, have maximum bite forces above 300 psi. A 37-year-old patient with a long history of bruxism recorded a maximum bite force of more than 990 psi (four to seven times normal).35
Fortunately, the bite force does not continue to increase in most bruxing patients. When muscles do not vary their exercise regimen, their size and function adjust to the dynamics of the situation. As a result, the higher bite forces and muscle size usually do not continue in an unending spiral.
Diagnosis
Bruxism does not necessarily represent a contraindication for implants, but it does dramatically influence treatment planning. The first step is to recognize the condition before the treatment is rendered. The symptoms of this disorder may be ascertained by a dental history and may include repeated headaches, a history (or presence) of fractured teeth or restorations, repeated uncemented restorations, or jaw discomfort upon awakening.22–36 Therefore, when the patient is aware of muscle tenderness or the spouse is conscious of the noise of bruxism during sleep, the diagnosis is readily obtained (Box 10-4). However, many patients do not attribute these problems to excessive forces on the teeth and report a negative history. A lack of these symptoms does not negate the possibility of bruxism.
Fortunately, many clinical signs warn of excessive grinding. The signs of bruxism include an increase in size of the temporalis and masseter muscles. These muscles and the external pterygoid may also be tender during palpation. In addition, other signs include deviation of the lower jaw on opening, limited occlusal opening, increased mobility of teeth, cervical abfraction of teeth, fracture of teeth or restorations, and uncemented crowns or fixed prostheses.35
A physical examination for the implant candidate should include palpation of the muscles of mastication. The masseter and temporalis muscles are easily examined during the initial appointment. Hyperactive muscles are not always tender, but tender muscles in the absence of trauma or disease is a sign of excess use or incoordination among muscle groups. The lateral pterygoid muscle is more often overused by the bruxing patient but is difficult to palpate. The ipsilateral medial pterygoid muscle provides more reliable information in this region. It acts as the antagonist to the lateral pterygoid in hyperfunction and, when tender, provides a good indicator of overuse of the lateral pterygoid.37 However, the most effective method to diagnose bruxism is to evaluate the wearing of the natural teeth23 (Box 10-5).
Nonfunctional wear facets on the incisal edges occur most often on natural teeth rather than on crowns made of porcelain or metal occlusals, especially in the anterior mandible and maxillary canines. Enamel opposing enamel causes more occlusal material wear than almost any other combination (e.g., enamel opposing metal, metal opposing metal, etc.).38 As a result, in a partially edentulous patient, enamel wear is easily observed in the bruxing patient.
Not only is enamel wear the easiest method to determine bruxism in a dentate patient, but Misch has noted the disorder may also be classified as absent, mild, moderate, or severe.23,39,40 No anterior wear patterns in the teeth signifies an absence of significant bruxism. Mild bruxism has slight wearing of anterior teeth but is not a cosmetic compromise (Figure 10-1). Moderate bruxism has obvious anterior incisal wear facets but no posterior occlusal wear pattern (Figure 10-2). Severe bruxism has an absence of incisal guidance as a result of the excessive wear, and posterior wearing of the teeth is obvious (Figure 10-3).




Tooth wear is most significant when found in the posterior regions and changes the intensity of bruxism from the moderate to the severe category. Posterior wear patterns are more difficult to manage because they are usually related to a loss of anterior guidance in excursions, and when the posterior teeth contact in excursive jaw positions, greater forces against the teeth are generated.41 The masseter and temporalis muscles contract when posterior teeth contact. With incisal guidance and an absence of posterior contact in a lateral excursion of this jaw, two thirds of these muscles do not contract and, as a consequence, the bite force is dramatically reduced. However, when the posterior teeth maintain contact, the bite forces are similar in excursions, as during posterior biting. Therefore, in a patient with severe bruxism, the occlusal plane or the anterior incisal guidance may need modification to eliminate all posterior contacts during mandibular excursions before the implant restoration.
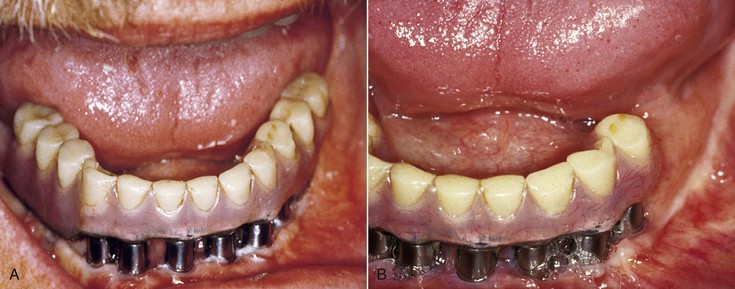
Bruxing patients often repeat the same mandibular movements, which are different from border movements of the mandible and are in one particular direction. As a result, the occlusal wear is very specific and primarily on one side of the arch or even on only a few teeth (Figure 10-4). This engram pattern usually remains after treatment. If the restoring dentist reestablishes incisal guidance on teeth severely affected by an engram bruxing pattern, the incidence of complications on these teeth will be increased.

The most common complications on teeth restored in this “pathway of destruction” are porcelain fracture, uncemented prostheses, and root fracture.35 When implants support the crowns in the “pathway of destruction,” the implant may fail; fracture; or have crestal bone loss, abutment screw loosening, porcelain fracture, or unretained restorations.39,40 If the patient continues the severe bruxism pattern, the question is not whether but when and which complications will occur. The dentist should tell the patient that these parafunctional habits will cause these problems. Treatment may be rendered to repair these problems, but there will be complications if the bruxism is not reduced.
Bruxism changes normal masticatory forces by the magnitude (higher bite forces), duration (hours rather than minutes), direction (lateral rather than vertical), type (shear rather than compression), and magnification (four to seven times normal).39,40 The method to restore severe bruxism may be problematic even when the desire is primarily cosmetic. As the anterior teeth wear, they may erupt, and the overall occlusal vertical dimension (OVD) remains unchanged. In addition, the alveolar process may follow the eruption of the tooth. As such, when the anterior teeth are restored for esthetics (or to obtain an incisal guidance), the reduced crown height cannot be increased merely by increasing the height of the crown to an average dimension.37 However, in some patients, the teeth do not erupt as they wear, and the vertical occlusal dimension does decrease. Therefore, the severe wearing diagnosis must include the evaluation of the OVD. The following guidelines are suggested:
1. Determine the position of the maxillary incisor edge of the anterior teeth. They may be acceptable (if eruption occurred as they wore) or need greater coronal length to correct related incisal wear. The maxillary incisal edge should be in the proper position (either remain as present if acceptable or restore if not acceptable) (Figure 10-5, A).

2. Determine the desired OVD. This is not an exact dimension and may exist at several different positions without consequence. However, similar to most factors, there is a range that is patient specific and does follow guidelines. The most common methods to determine this dimension relate to facial measurements, closest speaking space, physiologic rest position, speech, and esthetics (Figure 10-5, B to D). This is one of the most important steps. If the vertical dimension is collapsed because of anterior and posterior occlusal wear, much more rehabilitation is required. This condition is observed more often when bruxism is severe, the anterior incisal guidance was lost, and, as a consequence, the severe bruxism wear is increased due to an increase in force factors. The accelerated occlusal wear may cause a loss of OVD. The OVD is rarely decreased when incisal guidance is still present because the posterior teeth maintain the dimension and the anterior teeth have time to erupt because the forces are less and the wear rate is slower.
3. Evaluate and restore the position of the lower anterior teeth where necessary. In the past, it has been stated that a reconstruction of the mouth begins with the lower anterior teeth.37 However, the mandibular arch cannot be restored until the maxillary anterior teeth and OVD are established. Many esthetic and speech guidelines are available to help the restoring dentist with the position of the maxillary anterior teeth. For example, when a dentist begins the restoration of a completely edentulous patient, the maxillary anterior wax rim position is often first determined for similar reasons.
With natural teeth, the position of the lower anterior teeth should contact the lingual surfaces of the maxillary anterior teeth at the established OVD, and the amount of vertical overlap of the maxillary incisal edge and the angle of the incisal contacts in protrusive movements of the mandible determines the angle and height of the anterior guidance.37 This dimension must be greater than the condylar disc assembly (the angle of the eminentia) so the posterior teeth will separate during mandibular excursions.
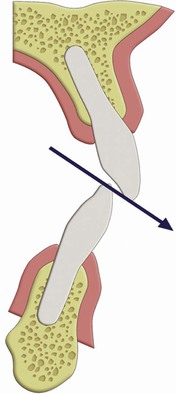
In patients with moderate to severe bruxism, the height of the vertical overjet and the angle of incisal guidance should not be extreme because the amount of the force on the anterior abutments, cement seals, and porcelain is directly related to these conditions (Figure 10-6). In other words, the greater the incisal overjet, the greater the distance between the posterior teeth in excursions and the greater the force generated on the anterior teeth during this movement. In patients with severe bruxism, the intensity of the force on the anterior teeth should be reduced because the duration of the force is increased.
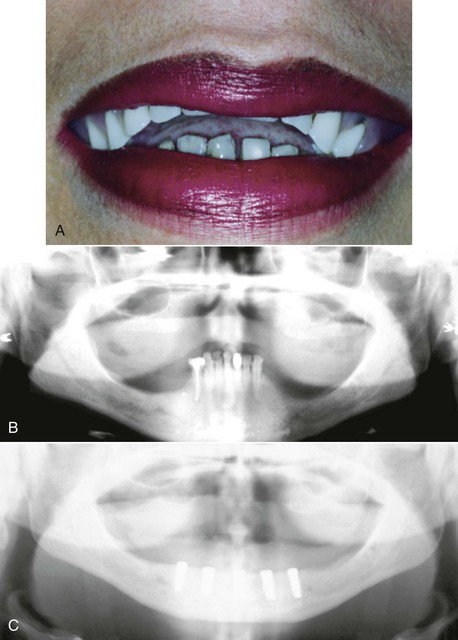
When anterior tooth wear is accompanied by tooth eruption and maintenance of the OVD and alveolar bone in the region has extruded toward the incisal plane, the worn incisal edges of the teeth are not the only thing to be restored. The alveolar bone and cervical regions should be reduced, and crown lengthening should be performed on the teeth before their restoration. This is most often necessary in the mandibular anterior region when the lower anterior teeth are opposing a denture but may be observed in any region of the mouth after long-term severe bruxism. In addition, endodontic therapy may be required to allow proper anterior tooth preparation. In a combination syndrome with a mandibular class I partial denture opposing a denture, the lower anterior teeth may need to be extracted in order to obtain the correct incisal edge position (Figure 10-7).
Fatigue Fractures
The increase in duration of the force is a considerable problem. Materials follow a fatigue curve, which is affected by the number of cycles and the intensity of the force42,43 (Figure 10-8). A force can be so great that one cycle causes a fracture (e.g., a karate blow to a piece of wood). However, if a lower force magnitude repeatedly hits an object, the object will still fracture. The wire coat hanger that is bent does not break the first time, but repeated bends will fracture the material—not because the last bend was more forceful but because of fatigue.

A bruxing patient is at greater risk of fatigue fractures for two reasons. The magnitude of the forces increases over time as the muscles become stronger and the number of cycles increases on the prosthetic components. Eventually, one of the components (implant, screw, abutment, prosthesis) will break if the parafunction cannot be reduced in intensity or duration (Figure 10-9). No long-term prosthetic result is expected in patients with severe bruxism. Therefore, when the implant dentist has identified the sources of additional force on the implant system, the treatment plan is altered in an attempt to minimize the negative effect on the longevity of the implant, bone, and final restoration. All elements able to reduce stress or modify the fatigue factor should be considered.
Porcelain fracture is of particular concern with the implant prosthesis in a bruxing patient (Figure 10-10). In a report by Kinsel and Lin, 34% of patients with bruxism experienced porcelain fracture, and more than 15% of crowns in bruxing patients fractured porcelain.44 When group function was used to restore these patients in lateral excursions, more than half of the patients experienced porcelain fracture with their implant prosthesis. Hence, it is appropriate in this category of patients to inform them of the porcelain fracture risk, use metal occlusal surfaces in nonesthetic regions, and use implant-protective occlusion concepts (which restore incisal guidance).

Occlusal Guards
The cause of bruxism is multifactorial and may include occlusal disharmony.37 When an implant reconstruction is considered in a bruxing patient, occlusal analysis is warranted. Premature and posterior contacts during mandibular excursions increase stress conditions.45 An elimination of eccentric contacts may allow recovery of periodontal ligament health and muscle activity within 1 to 4 weeks. Occlusal harmony does not necessarily eliminate bruxism, but this is no reason not to perform an occlusal analysis and eliminate the premature contacts. No study demonstrates an increase in parafunction after occlusal adjustment. Therefore, the ability to decrease the risk of occlusal overload on particular teeth and the added benefit of perhaps reducing parafunction is warranted in almost every patient diagnosed with a parafunctional habit of bruxism or clenching.
A night guard can be a useful diagnostic tool to evaluate the influence of occlusal disharmony on nocturnal bruxism. The Michigan night guard exhibits even occlusal contacts around the arch in centric relation occlusion and provides posterior disocclusion with anterior guidance in all excursions of the mandible.46 This device may be fabricated with 0.5- to 1-mm colored acrylic resin on the occlusal surface. After 4 weeks of nocturnal wear, the muscles and periodontal ligament are restored. If the patient wears this device for an additional month or more, the influence of occlusion on the bruxism may be directly observed because there are no premature contacts while the device is worn. If the colored acrylic is still intact, the nocturnal parafunction has been reduced or eliminated. Therefore, occlusal reconstruction or modification may proceed. If the colored acrylic on the night guard is ground through, an occlusal adjustment will have little influence on decreasing this parafunctional habit. The night guard is still indicated to relieve stresses during nocturnal parafunction, but the treatment plan should account for the greater forces.
Forces from moderate to severe bruxism are the most difficult to address on a long-term basis. Education and informed consent of the patient are helpful to gain cooperation in eliminating or reducing the noxious effects. If the opposing arch is a soft tissue–supported removable prosthesis, the effects of the nocturnal habit may be minimized if the patient removes the prosthesis at night. The use of a night guard is helpful for a patient with a fixed prosthesis in order to transfer the weakest link of the system to the removable acrylic device. Centric contacts in centric relation occlusion and anterior-guided disocclusion of the posterior teeth in excursions are strongly suggested on the night guard, which may be designed to fit the maxilla or mandible.
Unlike teeth, implants do not extrude in the absence of occlusal contacts. As a result, in partially edentulous patients, the maxillary night guard can be relieved around the implant crowns so the remaining natural teeth bear the entire load.23,39 For example, for a maxillary central implant restoration, the night guard is hollow over the restoration so no occlusal force is transmitted to the implant crown (Figure 10-11). When the restoration is in the mandible, the occluding surfaces of the maxillary night guard are relieved over the implant crowns so no occlusal force is transmitted to the implants (Figure 10-12).


A mandibular posterior cantilever on a full-arch implant prosthesis may also be taken out of occlusion with a maxillary night guard. When a posterior quadrant of implants supports a fixed prosthesis in the maxilla opposing mandibular teeth, a soft reline material may be placed around the implant crowns to act as a stress relief element and decrease the impact force on the restoration (Figure 10-13). When full-arch implant restorations are opposing each other, the night guard provides solely anterior contacts during centric occlusion and mandibular excursions (Figure 10-14). Thus, the parafunctional force is reduced on the anterior teeth and implants and eliminated in the posterior regions.


Treatment Planning
The implant treatment plan is modified primarily in two ways when implants are inserted in the posterior region with severe bruxism: (1) additional implants that are wider in diameter are one method used to reduce the overload risk, and (2) the anterior teeth may be modified to re-create the proper incisal guidance and avoid posterior interferences during excursions. The elimination of posterior lateral occlusal contacts during excursive movements is recommended when opposing natural teeth or an implant or tooth-supported fixed prosthesis. This is beneficial in two aspects: (1) because lateral forces dramatically increase stress at the implant–bone interface, the elimination of posterior contacts diminishes the negative effect of angled forces during bruxism,46,47 and (2) the presence of posterior contacts during excursions, and almost all fibers of the masseter, temporalis, and the external pterygoid muscles contract and place higher forces on the anterior teeth and implants. On the contrary, during excursions in the absence of posterior contacts, fewer fibers of the temporalis and masseter muscles are stimulated, and the forces applied on the anterior implant–teeth system are reduced by as much as two thirds.41
Clenching
Clenching is a habit that generates a constant force exerted from one occlusal surface to the other without movement. The habitual clenching position does not necessarily correspond to centric occlusion. The jaw may be positioned in any direction before the static load; therefore, a bruxing and clenching combination may exist. The clench position most often is in the same repeated position and rarely changes from one period to another. The direction of load may be vertical or horizontal. The forces involved are in significant excess of normal physiologic loads and are similar to bruxism in amount and duration; however, several clinical conditions differ in clenching.48,49
Diagnosis
Many clinical symptoms and signs warn of excessive grinding. However, the signs of clenching are often less obvious. The forces generated during clenching are usually directed more vertically to the plane of occlusion, at least in the posterior regions of the mouth. Wearing of the teeth is usually not evident; therefore, clenching often escapes notice during the intraoral examination. As a result, the dentist must be more observant to the diagnosis of this disorder.29
Many of the clinical signs of clenching resemble bruxism. When a patient has a dental history or presence of muscle tenderness (often upon awakening) or tooth sensitivity to cold, parafunction is/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


