In this article, the authors examine the optimal time for dental placements in young individuals and emphasize the importance of ensuring skeletal maturity has been reached, except in some situations where dentoalveolar growth is expected to be minimal or where the value afforded by an anchored prosthesis outweighs the disadvantage of local growth inhibition. They offer examples of the difficulties encountered in implants placed in a growing individual, including loss of integration, diminishment of posterior function, and excessive wear or fracture of restorative materials in the anterior region. Because individual growth cessation varies by up to 6 years within each gender, chronologic age cannot be used as a guide in planning implants; rather, analysis of skeletal development can be made from carpal radiographs or from superimposition of serial lateral cephalograms.
The most appropriate earliest age for placement of dental implants is generally held to be the age at which skeletal growth is thought to cease. The end of adolescence and the beginning of young adulthood coincide with the exhaustion of growth potential, but adaptive changes of the jaws continue throughout life. Until recently it was thought that adaptation has little clinical effect on implants.
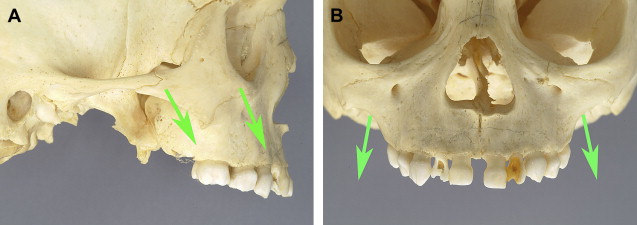
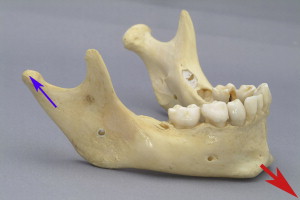
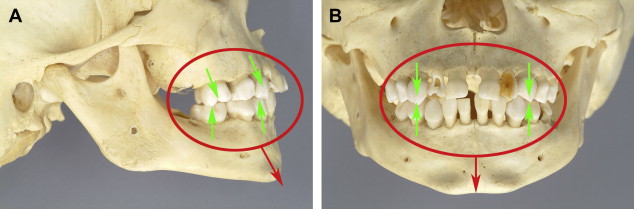
Growth of the maxilla is characterized by remodeling in a posterosuperior direction while simultaneously being displaced in the opposite anteroinferior direction ( Fig. 1 ). In contrast, growth of the mandible is characterized by displacement away from its articulation in the glenoid fossae as the condyles and rami relocate in a posterosuperior direction ( Fig. 2 ). Natural tooth movement occurs as a result of eruption and of being carried along passively with the maxilla and mandible, both of which undergo displacement anteroinferiorly during craniofacial morphogenesis ( Fig. 3 ). Tooth movement facilitates adaptation to changing anatomic relationships as the entire craniofacial assembly changes during this period of great flux.
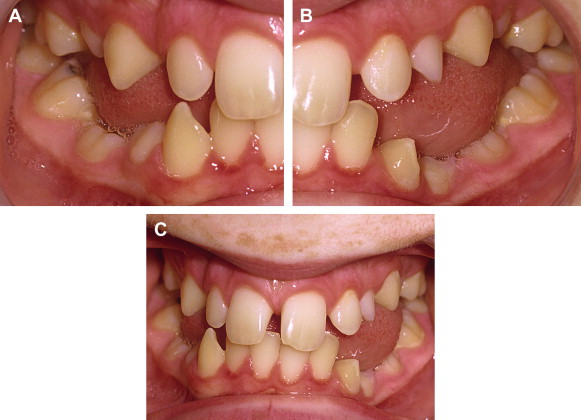
Experiments designed to study the effect of dental implants on dentoalveolar growth and development in pigs demonstrated that implants, owing to an absence of a periodontal ligament, behave like ankylosed teeth; that is, they remain stationary and do not erupt together with adjacent teeth ( Fig. 4 ). In failing to move together with erupting teeth, implants were found to inhibit local growth and development of the alveolar process. A 3-year prospective clinical study in adolescents with congenitally missing teeth verified that implants do not move during growth of the jaws, and undergo relative submergence of a magnitude proportional to the amount of residual jaw growth ( Fig. 5 ).
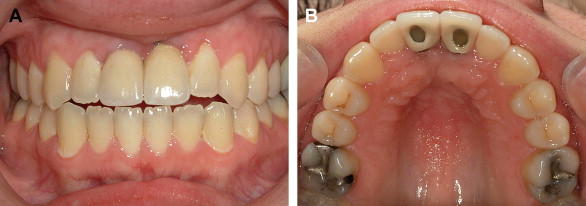
Submergence of an implant is disadvantageous for a number of reasons. First, an infraocclusion occurs, which disrupts carefully constructed occlusal relationships and leads to compensatory eruption of opposing teeth and tipping of adjacent teeth. Second, a vertical discrepancy develops between the mucosal margin of the implant and the gingival margins of adjacent teeth ( Fig. 6 ).
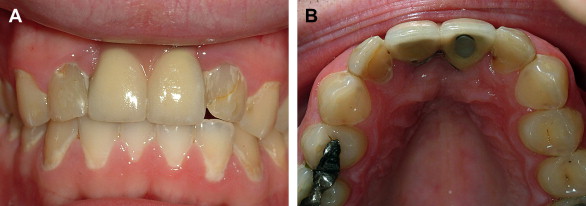
Submergence of an implant or an ankylosed tooth appears not to be a passive phenomenon; rather, it exerts an inhibitory effect on eruption of neighboring teeth, the force of which diminishes with distance. The distance over which this field effect is seen is usually restricted to one or two teeth on either side of a submerged implant, and depending on the degree of residual alveolar growth remaining at the time of implant placement, disruption of the occlusal plane can be severe (see Fig. 4 ; Fig. 7 ).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


