Figure 2.39 Panoramic radiograph showing abnormal patters over the right TMJ, zygomatic arch, and mandibular ramus.
F. Extraoral Status
Weight and height
- Within normal limits.
Facial asymmetry
- Asymmetry with diffuse preauricular swelling on the right side.
Neurologic findings
- Sensory paresthesia for touch and cold in the right mental region.
Motor function abnormalities
- Movement of the extremities is within normal limits.
Temporomandibular joint
- Palpation reveals elastic hard mass, 30 mm in diameter, in the right TMJ region.
- Palpation pain.
Masticatory muscles
- No palpation pain.
Jaw movement capacity
- Maximum unassisted mouth opening 32 mm.
- No mandibular movement pain.
Neck
- Within normal limits; no movement or palpation pain.
G. Intraoral Status
Soft tissues
- Within normal limits.
Hard tissues
- No caries, but restorations on several teeth.
Occlusion
- Within normal limits.
H. Additional Examinations and Findings
- CT (Figure 2.40a) and MRI scans (Figure 2.40b–d) show typical appearance of chondrosarcoma.
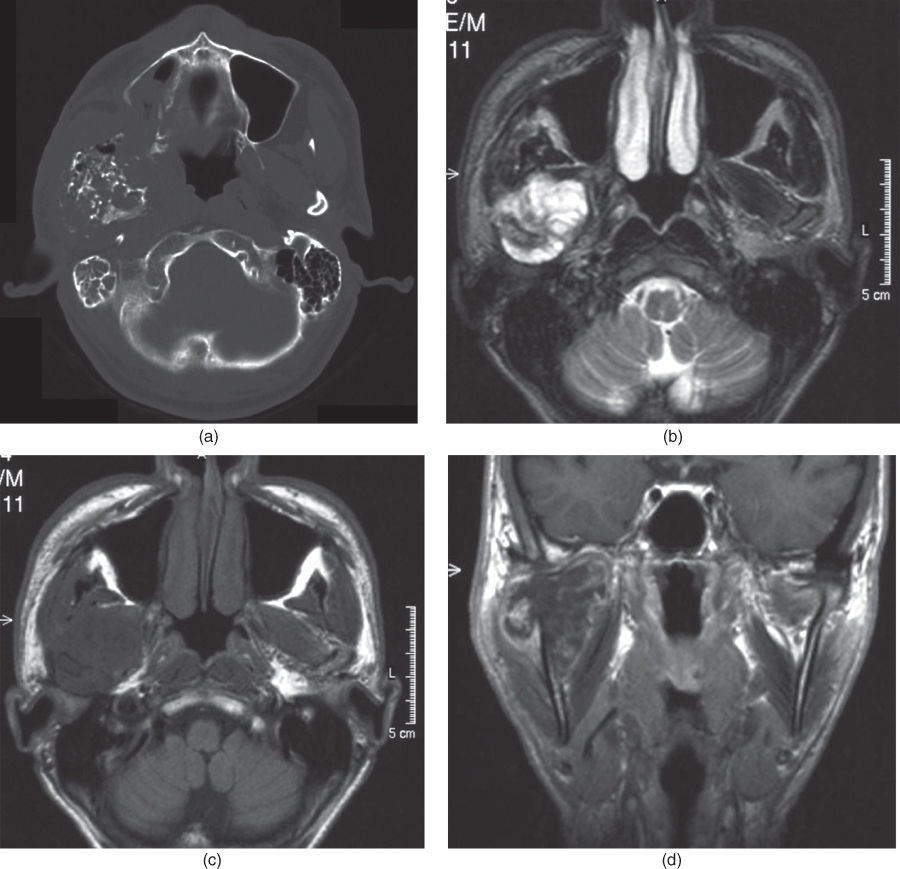
Figure 2.40 Images of the chondrosarcoma of the right condyle: (a) CT scan, (b) T2-weighted axial MRI image, (c) T1-weighted axial, and (d) coronal MRI images.
I. Diagnosis/Diagnoses
Expanded DC/TMD
- Malignant neoplasm in the TMJ.
Other
- Chondrosarcoma of the condyle.
J. Evidence-based Treatment Plan, including Aims
Aim
- Immediate removal of malign tissue.
Treatment
- Resection of the tumor.
K. Prognosis and Discussion
- Prognosis is poor regarding survival, especially in a high-grade lesion like this.
- Individualized treatment based on the principles of resection achieving clear margins and consideration of adjuvant radiotherapy or chemotherapy may improve the prognosis.
Background Information
- Chondrosarcoma of the head and neck is rare, although it constitutes 40% of the reported TMJ sarcomas. In terms of the bony skeleton, head and neck lesions account for only 1%.
- The production of malignant cartilage along with cellular pleomorphism are the hallmarks of the chondrosarcoma. No osteoid formation is observed.
- Histopathologically, cellularity is increased with a myxomatous matrix, and the cartilage cells tend to be large, and may contain multiple nuclei or a large nucleus (Figure 2.41).
- Chondrosarcoma develops from mesenchymal stem cells, which show partial chondroblastic differentiation. Typically, it is a slow-growing tumor and the majority is low grade.
- High-grade tumors may metastasize to regional lymph nodes. Low-grade tumors have an excellent prognosis, but recurrences are often observed.
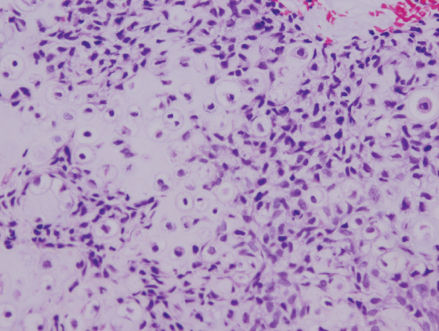
Figure 2.41 Histopathological finding of the chondrosarcoma. Cellularity is increased with a myxomatous matrix and the cartilage cells tend to be large. The cells may contain multiple nuclei or a large nucleus.
(Plesh et al., 2005)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


