Chapter 2
The first appointment
Orthodontic patients are usually referred by their own dentist (their general dental practitioner (GDP)) for specialist orthodontic treatment.
These referrals can be sent to:
- an orthodontic specialist practitioner
- a community orthodontist
- a consultant orthodontist
- a dental practitioner with special interest (DPwSI) and some basic training in orthodontics
Some adult patients may choose to self-refer.
The referring dentist may wish to send the patient to an orthodontist to:
- see and advise
- if there are teeth that are slow to erupt
- if there are teeth that have submerged
- if there are teeth that are in a self-damaging position
- see and monitor
- if the patient is dentally too young for treatment
- if there are already signs of adverse dental development, i.e. growth, facial asymmetry or crowding
- see and treat
- if the second dentition has developed but is overcrowded
- if there is a complex problem
- if there is a multi-disciplinary need
The referral letter needs to contain as much relevant information for the orthodontic practitioner as possible.
Apart from the basic data:
- name
- address
- telephone numbers (land, mobile, work, etc.)
- date of birth
- National Health number
- name of general practitioner (doctor)
it also needs to give:
- clinical reason for referral (what the dentist feels is the problem)
- medical history (if it is helpful to know in advance, e.g. attention deficit hyperactivity disorder, autism, deafness or dental phobia)
- dental history (good oral hygiene, high caries level, etc.)
- any previous orthodontic history (e.g. previous assessment or treatment)
- social history (e.g. supportive family, regular check-ups)
- what the patient/parent is concerned about (‘fangs’, teasing)
- whether the patient is concerned at all (quite happy to stay as they are)
- likely compliance (supportive family, patient keen)
When the referral letter is received, the patient (or their parent or guardian if they are underage) is sent an appointment.
On the first visit, a full orthodontic assessment is carried out (Figures 2.1 and 2.2).
This includes:
- checking the name and age of the patient
- finding out what is of concern to the patient
- full medical history, including whether the patient
- has allergies (nickel, latex, etc.)
- is currently under the care of a doctor for any reason
- has had any operations
- is taking medication of any kind
- has asthma, if so, type of inhalers
- has diabetes
- has or had chest or heart conditions
Patients and/or parents are asked to fill in and sign a health questionnaire form. This is updated and checked regularly.
It includes details of:
- school or college (day or boarding)
- work
- contact sports played
- musical instruments played by mouth
- any digit (thumb or finger) sucking, bruxism (tooth grinding)
THE CLINICAL ASSESSMENT RECORDS
These begin with extra-oral features and then move on to intra-oral ones.
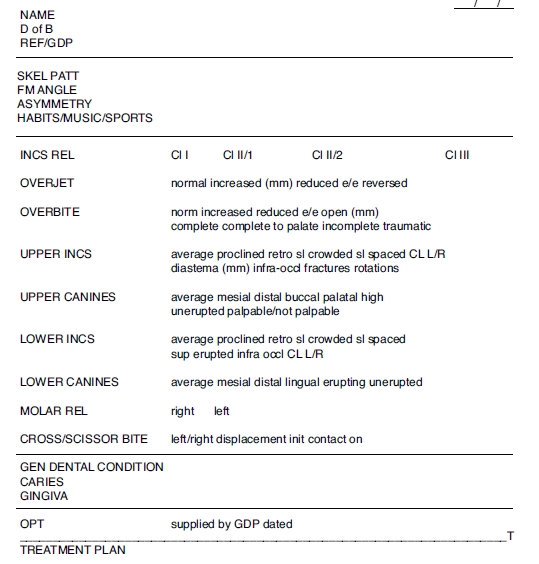
Figure 2.1 Sample of assessment form from a specialist orthodontic practice. (Reproduced with the kind permission of Alan Hall, South Downs Orthodontic Practice.)
Skeletal pattern
The maxilla-to-mandible relation in the antero-posterior plane:
- Class I
- Class II
- Class III
- mild
- moderate
- severe
Figure 2.2 Sample of assessment form from a hospital orthodontic department. (Reproduced with the kind permission of Jo Clark, Worthing and Southlands Hospitals NHS Trust.)
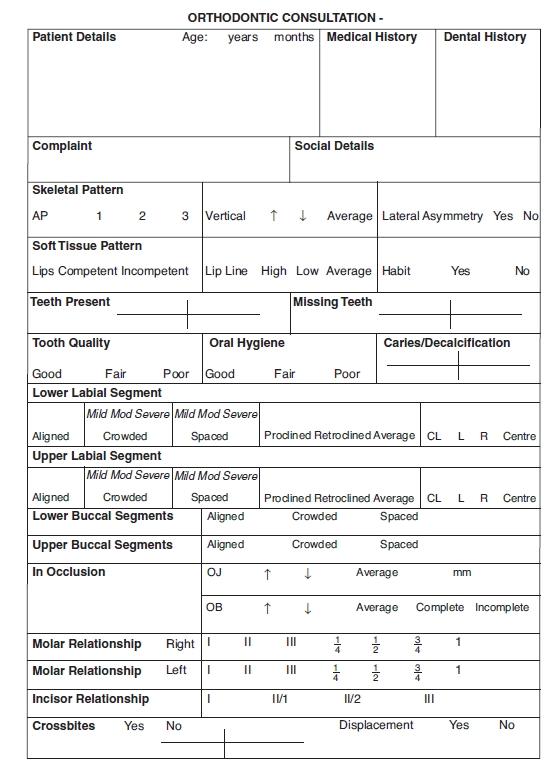
Figure 2.3 Drawing showing relation of FM angle.
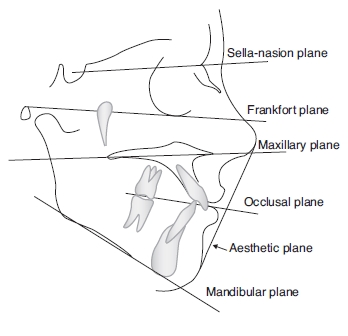
FM (Frankfort-mandibular) angle (Figure 2.3)
- high
- average
- low
Asymmetry
- This is usually mandibular
Soft tissues
- Lips
- line
- competency
- expressive behaviour
- if lower lip is behind upper incisors
(This is the end of the extra-oral examination.)
- Tongue
- size
- position in mouth
- swallowing behaviour
- Tonsils
- if there is a history of difficulties in breathing through the nose, snoring or repeated sore throats
- Frenum
- upper
- lower
Gingivae and oral hygiene
- health of the gums
- presence of plaque
Charting of the teeth
- present
- absent (unerupted or extracted)
- presence of caries/restorations/fissure sealant
- erosion
- enamel hypomineralisation
- hypoplasia
- size discrepancy, e.g.:
- microdont, small tooth (microdontia)
- megadont, large tooth (megadontia)
- supernumeraries – teeth which are additional to the norm:
- most often found in the anterior maxilla
- can be conical or tuberculate
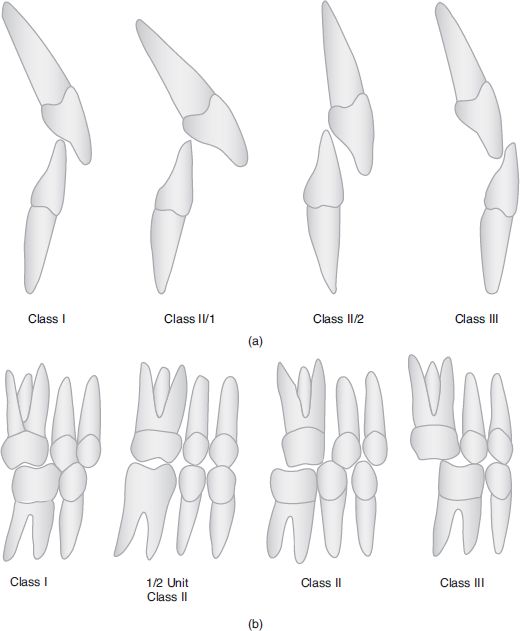
Incisor relationship (Figure 2.4a)
- Class I
- Class II/1
- Class II/2
- Class III
Overjet
Horizontal measurement between upper and lower incisors:
- normal (3 mm)
- increased (record the measurement in millimetres)
- edge to edge
- reversed
Overbite
- upper incisors overlap
Figure 2.4 Diagram of (a) incisor relationship and (b) buccal segment occlusion.
- lowers in vertical plane
- normal (3 to 4mm)
- increased
- reduced
- edge to edge
- open (record the measurement in millimetres)
- complete
- complete to palate
- incomplete
- traumatic
Upper and lower incisors
- average inclination
- proclined
- retroclined
- crowded
- rotations
- spaced
- diastema (record space in millimetres)
- centre line
- infra-occluded
- supra-erupted
- any fractures/restorations
- any abnormal mobility
- mesial or distal inclination
- buccal or palatal/lingual
Upper canines
- average inclination
- high
- unerupted but palpable
- unerupted but not palpable
- mesial or distal
- buccal or palatal
Lower canines
- average inclination
- mesial
- distal
- buccal
- lingual
- erupting
- unerupted
Molar relationship (buccal segment occlusion) (Figure 2.4b)
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


