Introduction
The aim of this study was to evaluate clinically, radiographically, and histologically orthodontic tooth movement into bone regenerate after mandibular distraction osteogenesis to elucidate the optimal timing for initiating tooth movement.
Methods
The study sample consisted of 9 male mongrel dogs. An average edentulous space of 9 mm was created by using a custom-made bone-borne distractor fixed on the mandibular corpus of each dog. The dogs were equally divided into 3 groups, and tooth movement began into the distraction gap after 1, 3, or 6 weeks of consolidation. The rate and type of tooth movement as well as the adverse tissue reactions (root resorption and crestal bone loss) were evaluated.
Results
Radiographic and histologic analyses showed analogous adverse tissue reactions in association with early tooth movement into the regenerate bone. Furthermore, the rate and type of tooth movement were variable in the 3 groups.
Conclusions
Early tooth movement into the distraction regenerate is not recommended because it could result in adverse tissue reactions. Moreover, radiographic examination of the distraction regenerate is advisable and could be used as a guide before starting tooth movement.
Distraction osteogenesis (DO) is the process of generating new bone in a gap between 2 bone segments in response to the application of graduated tensile stress across the bone gap. The DO surgical concept was introduced by Codivilla in 1905 and implemented 50 years later by Ilizarov. DO has opened new horizons for the orthodontist in treating crowded dental arches, especially those associated with craniofacial anomalies.
In most of the current mandibular osteodistraction reports, the osteotomies are done in nontooth-bearing areas posterior to the alveolar process with lengthening of the ramus and the body as the common target. On the other hand, fewer studies reported midline interdental osteotomies for transverse mandibular expansion, particularly in patients with severe anterior dental crowding. In general, avoidance of osteotomies in the tooth-bearing body of the mandible is partly the result of the limited data about the consequences of reconstructing the interdental gaps created after distraction by either orthodontically moving teeth or placing implants into the newly formed bone.
Although the clinical possibility of moving teeth into regenerate alveolar bone is no longer disputed, the timing of initiating orthodontic tooth movement into the newly created bone remains a topic of discussion. Some authors suggested that tooth movement should not begin until the regenerate bone has consolidated for 8 to 12 weeks. However, others have shown that tooth movement can begin much earlier in the consolidation period. This study was designed to evaluate clinically, radiographically, and histologically orthodontic tooth movement into bone regenerate created after mandibular DO to elucidate the optimal timing for starting tooth movement.
Material and methods
The sample for this study consisted of 9 adult male mongrel dogs with an average weight of 13 to 17 kg, aged 11 to 15 months. In all dogs, osteotomies for distraction were done in tooth-bearing areas of the mandible between the third and fourth premolars. The dogs were divided equally into 3 groups based on the time of initiating tooth movement into the regenerate bone created after distraction. Tooth movement began after 1, 3, and 6 weeks of consolidation in groups I, II, and III, respectively, and continued for 8 weeks or until complete contact between the third and fourth premolars. Bilateral mandibular distraction was done in all dogs, except for 1 dog in each group that had only unilateral mandibular distraction. This dog was killed before tooth movement to examine the quality of the formed regenerate at that time.
In this study, a custom-made intraoral bone-borne distractor was used that was made up of a rapid palatal expander (Forestadent, Pforzheim, Germany), 2/0 straight stainless steel surgical miniplates (KLS Martin, Jacksonville, Florida), and 6 titanium bone screws (11 mm) for bicortical fixation ( Fig 1 ).
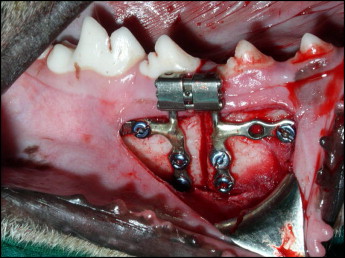
The surgical protocol was as follows: An intraoral soft-tissue 4-cm vestibular incision was made from the second premolar to the first molar with a number 15 blade. A mucoperiosteal flap was reflected inferiorly, exposing the inferior border of the mandible with minimal dissection superiorly enough to expose the area of the planned osteotomy and to maintain the integrity of the gingival tissue. A mandibular buccal osteotomy was initiated by using a reciprocating saw blade, and then the device was fixed in place with 3 bicortical miniscrews on each side of the osteotomy. The osteotomy was completed by using a spatula osteotome. The osteotomy was made closer to the fourth premolar; this resulted in root injury in some dogs. This was done to provide enough bone coverage distal to the third premolar root and to prevent its possible injury during the osteotomy procedure ( Fig 1 ). The mucosal flap was then closed with a continuous 3-0 polyglactin 910 suture. An indentation was made on the middle of the labial surface of the canine with a round bur to be used as a distant reference point for monitoring the amount and rate of tooth movement. The other reference point was the tip of the crown of the third premolar.
The distraction protocol was as follows: The dogs were carefully monitored after surgery. Oral chlorhexidine was used for irrigation twice daily for 4 days postoperatively and when signs of inflammation were observed.
The bone segments were maintained in a neutral position for 7 days (latency period). On the eighth postoperative day, activation of the appliance began at a rate of 1 mm per day divided into 2 increments of 0.5 mm for 12 days followed by either 1, 3, or 6 weeks of consolidation before initiating tooth movement. In all animals, the device was maintained in position during tooth movement.
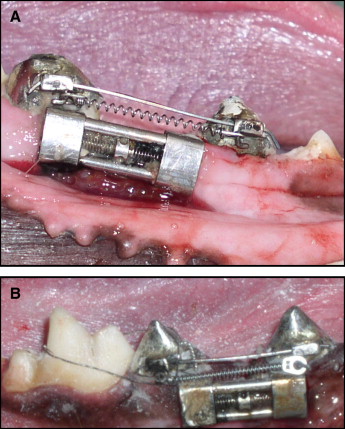
The tooth movement protocol was as follows: Custom-made crowns for the third and fourth premolars were fabricated. On the labial surface of each already prepared crown, a stainless steel molar tube (0.022 × 0.028 in) was soldered in such a way that it allowed a high-gauge straight stainless steel wire (0.019 × 0.025 in) to slide through freely. The crowns were cemented with glass ionomer cement. A calibrated nickel-titanium coil spring with a force of 150 g was attached to the hooks of the soldered molar tubes to move the third premolar into the edentulous segment created by distraction. Meanwhile, the fourth premolar was prevented from movement by ligation with the first molar with a ligature wire ( Fig 2 ).
All animals were monitored postsurgically for wound dehiscences, infection, and loosening or breakage of the distractor.
At the end of the distraction phase, the amount of distraction on each side was measured from the tip of the third premolar crown to the tip of the fourth premolar crown by using a sliding caliper.
During the tooth movement phase, the distance from the third premolar crown tip and the indentation made on the middle of the labial surface of the canine of the same side was measured at the start of tooth movement and repeated every 2 weeks for 8 weeks to estimate the amount and rate of tooth movement in each group.
At the end of the experiment in each group, the dogs were humanely killed with an intravenous overdose of pentobarbital (40-50 mg/kg).
Digital periapical radiographs were then taken for the hemi-mandibles by using phosphor storage plates (Digora, Soredex,Tuusula, Finland). The radiographs were evaluated for signs of new bone formation in the distraction gaps. Moreover, the densities of the formed regenerate bone in each group were measured at the proximal ends of the osteotomized segments as well as at the center of the newly formed bone and compared by using software (Digora for Windows, version 2.5; Soredex).
The tissues were prepared as follows. The mandibular segments including the fourth premolar, distracted new bone, and the third premolar were dissected en bloc. The specimens were processed according to the method of Callis. After complete decalcification, the specimens were embedded in paraffin with the conventional technique, and sagittal serial sections, 6 μm thick, were stained with hematoxylin and eosin for examination.
Statistical analysis
The amounts and rates of tooth movement in the 3 groups were analyzed and compared by using analysis of variance (ANOVA) followed by Scheffé post-hoc tests. Statistical significance was established at a P value of 0.05.
Results
Throughout this experiment, all animals tolerated the surgical procedures well, ate without problems, and consistently gained weight postoperatively.
During the latency period, 3 cases of wound dehiscence were observed in 3 animals. No infections were reported, and the dehiscences were managed with oral chlorhexidine irrigation twice daily until complete healing.
In all animals, the area between the distractor and the buccal mucosa was perceived to be an area of food stagnation, and it was difficult to maintain good hygiene. Accordingly, in some cases (6 of 15 distraction sites; 2 in group I, 1 in group II, and 3 in group III), a slight buccal gingival inflammation was observed at the area of distraction and was managed by oral chlorhexidine irrigation twice daily until complete resolution of the inflammation.
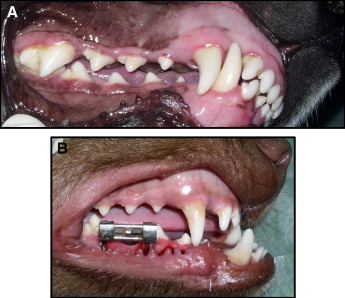
At the end of the distraction phase, all animals with bilateral mandibular distraction developed increased prognathism of the mandible compared with the maxilla. The increase in the sagittal body of the mandible concomitant with distraction accompanied the creation of an edentulous segment with an average of 9.02 ± 2.42 mm as measured from the tip of the third premolar crown to the tip of the fourth premolar crown. It was observed that in all cases the edentulous alveolar ridge created by distraction had a saddle-shaped appearance. Furthermore, all dogs with unilateral mandibular distraction developed a unilateral mandibular shift to the contralateral side that was obvious clinically ( Fig 3 ).
With progressive retraction of the third premolars at the time planned for each group, the teeth were successfully moved distally about two thirds of the length of the created edentulous space, except in group I where the teeth moved only about one third of the length of the edentulous space. The premolars were distalized about 3.65 ± 0.95 mm in group I, 9.38 ± 2.04 mm in group II, and 7.72 ± 2.04 mm in group III. The rate of tooth movement was steady over the 8 weeks of the experiment in all groups, except in group II where it increased in the last 4 weeks of tooth movement. The rates of tooth movement were about 0.46 ± 0.12 mm per week for group I, 1.17 ± 0.26 mm per week in group II, and 0.97 ± 0.26 mm per week for group III ( Table I ).
| Mean ± SD (mm) | |||
|---|---|---|---|
| Amount | Rate (weeks 0-4) | Rate (weeks 4-8) | |
| Group I | 3.65 ± 0.95 | 0.44 ± 0.13 | 0.48 ± 0.08 |
| Group II | 9.38 ± 2.04 ∗ | 1.07 ± 0.25 | 1.27 ± 0.17 |
| Group III | 7.72 ± 2.04 ∗ | 1.03 ± 0.49 | 0.9 ± 0.11 |
∗ The rates were significantly greater in groups II and III ( P <0.05) than in group I.
The rates of tooth movement were significantly greater in groups II and III ( P <0.05) than in group I ( Fig 4 ).

In this study, attempts to use rigid sliding mechanics for orthodontic tooth movement did not guarantee pure bodily movement in all situations. The results of this experiment showed severe tipping movements in 3 of 4 premolars in group II, with the fourth one showing moderate tipping during retraction into the distraction regenerate. On the other hand, all premolars in groups I and III demonstrated bodily movement, with the exception of 1 premolar in group I that had a severe tipping movement during retraction into the regenerate bone.
Radiographs taken for the distraction gap after 1 week of consolidation (group I) showed sharp demarcations of the osteotomy line. The distraction gap appeared to be mostly radiolucent with areas of radiopacities indicating new bone starting to form at the osteotomized end of the segments proceeding toward the center of the distraction gap ( Fig 5 , A ).
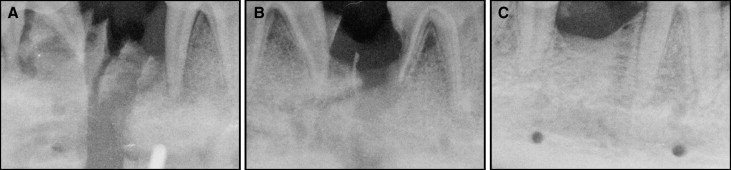
After 3 weeks of consolidation (group II), the osteotomy line started to be less evident with an increase in radiopacity of the distraction gap, denoting further extension of bone formation ( Fig 5 , B ).
After 6 weeks of consolidation (group III), the distraction gap had a saddle-shaped appearance and was perceived to be homogenously radiopaque and indistinguishable from the host bone ( Fig 5 , C ).
When we compared bone density measurements among the groups, we found a gradual increase in the bone density of the distraction regenerate concomitant with the increase in the consolidation period; this in turn reflected the increase in mineralization ( Table II ).
| Proximal end | Central area | Distal end | |
|---|---|---|---|
| Group I | 155.77 | 145.02 | 156.33 |
| Group II | 163.31 | 156.78 | 158.85 |
| Group III | 176.30 | 167.19 | 176.30 |
Radiographic evaluation after tooth movement into the distraction regenerate in group I showed severe external apical and lateral resorption of the distal root of the third premolar with loss of the lamina dura. Meanwhile, an irregular band of radiolucency was observed at the center of the distraction gap, denoting incomplete mineralization of the distraction regenerate at that time. It was noticed that the third premolar maintained an upright position while moving into the distraction gap. At the same time, moderate to severe crestal bone loss was detected with preservation of the interseptal bone ( Fig 6 , A ).

In group II, there was mild root resorption with preservation of the lamina dura especially in the area of the root apex. The distraction regenerate was more or less indistinguishable from the host bone at that time, indicating greater regenerate mineralization than in group I. In this group, the tipping type of tooth movement was manifested with mild reduction in crestal bone levels ( Fig 6 , B ).
In group III, there was no radiographically detectable root resorption with preservation of the lamina dura. Similar to group II, the distraction regenerate was indistinguishable from the host bone, indicating progressive regenerate mineralization. In this group, bodily tooth movement was manifested despite the greater distance of tooth movement than in group I ( Fig 6 , C ).
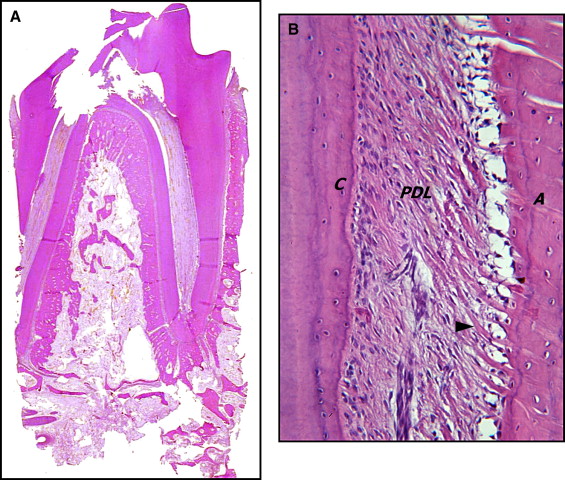
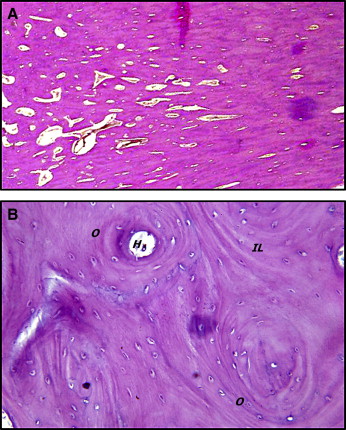
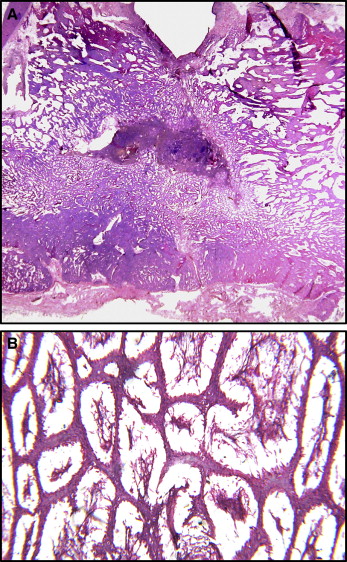
The histologic appearance of the canine mandible bones was normal ( Fig 7 ). The control bone biopsy sample showed regular lamellar structure with well-developed interstitial lamella and haversian canaliculi. Additionally, organized osteon structures were observed in the section with multiple trapped osteocytes in calcified matrix. Neither osteoclasts nor osteoblasts were observed in the haversian canaliculi. On the other hand, some medium-sized vessels were detected.
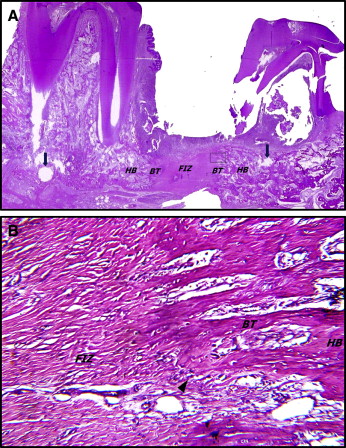
Examination of the histologic appearance of the distraction regenerate in group I ( Fig 8 ) showed a gap filled with fibrovascular tissue comprising most of the total regenerate area and organized as centrally arranged collagen bundles with interspersed vascular channels. No evidence of cartilage tissue was seen in the distraction gap. On the other hand, there was some evidence of new bone formation as small areas of bone trabeculae at the host bone margins oriented parallel to the direction of distraction with widely interspersed bone marrow spaces. Furthermore, the upper border of the distraction regenerate displayed the typical saddle-shaped appearance that was evident both clinically and radiographically.
The histologic appearance of the distraction regenerate in group II ( Fig 9 ) showed more progression toward maturation with marked reduction in the dimension of the fibrous interzone; it was wider at the upper than at the lower part of the regenerate. The newly formed bone maintained the parallel orientation of trabeculae to the direction of distraction, particularly near the lower border adjacent to the inferior cortex.
The newly formed bone appeared more mature and less vascularized than that in group I. Small islands of cartilage tissue were observed in the subapical region of the distraction regenerate close to the inferior alveolar canal. The chondrocytes of this cartilage tissue were arranged in an irregular pattern with no clearly defined cellular orientation.
There was no significant difference in osteogenesis between the proximal and distal segments of the mandible. On the other hand, bone regeneration seemed to be more pronounced in the lower portion compared with the upper part of the mandible.
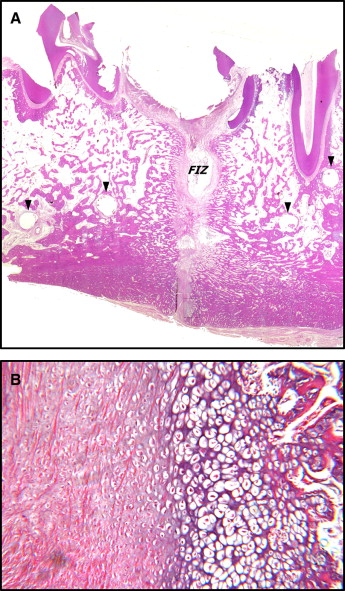
The histologic appearance of the distraction regenerate in group III ( Fig 10 ) showed further progression toward maturation accompanied by complete obliteration of the fibrous interzone with newly formed bone trabeculae interspersed with wide marrow spaces.
At this stage, a network of thin trabeculae of newly formed nonlamellar bone was observed. These trabeculae occupied most of the distraction gap and did not display the parallel arrangement to the distraction vector. The newly formed trabeculae were lined by osteoblasts arranged in a palisading manner and were laying down an osteoid matrix. On the other hand, more mature lamellar bone was found near the lower border of the mandible with no evidence of cartilage tissue at this stage.
The histologic appearance of the periodontal structures of the third premolar of the canine model before attempting tooth movement was normal ( Fig 11 ).