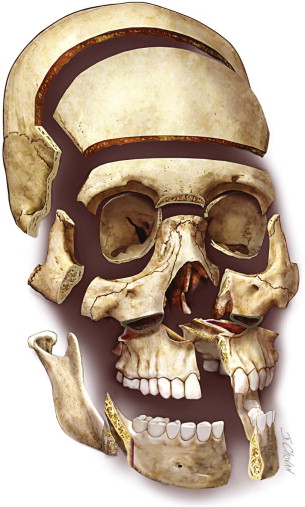
Adaptations and improvements in maxillofacial osteotomies have changed the spectrum of skull base surgery. Imaging, endoscopic and open techniques, embolization, navigation, focused radiation therapy, and infection control have all improved the outcomes in surgery of the skull base. Certain tumors require an open approach. The expertise of maxillofacial surgeons in trauma, corrective, cosmetic, and reconstructive surgery of the craniofacial complex allows for expanded options in providing wide field exposure for skull base surgery. Many tumors of the skull base cross anatomic boundaries, as is seen with invasion of the orbit, frontal, ethmoid, and sphenoid sinuses. Creative planning and surgical exposure are imperative. The goals of treatment are to remove the tumor safely and to provide reconstructive options for the complex residual deformity. Endoscopic and minimum incision access can limit exposure for large, complex lesions in difficult anatomic locations. Common osteotomy techniques for maxillofacial procedures can easily be used for wide field cranial base access. ( Figure 49-1 ) These access osteotomies are related procedures that use the same instrumentation and can be used for multiple purposes, even in combination. ( Fig 49-2 )
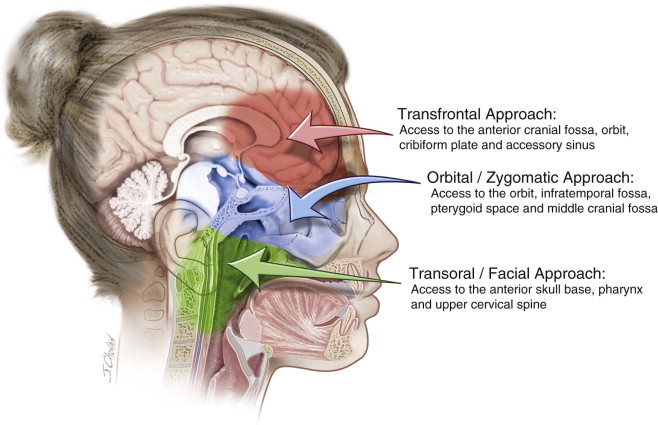
Transfrontal Approach: Access to the Anterior Cranial Fossa, Orbit, Cribriform Plate, and Accessory Sinuses
Armamentarium
History of the Procedure
The transfrontal approach, involving removal of the supraorbital bar combined with a bifrontal craniotomy, is used for multiple conditions, including congenital deformities, frontobasilar trauma, and tumors of the anterior cranial fossa. The advantage of this method is the direct low approach, which limits the retraction of the frontal lobe.
Indications for the Use of the Procedure
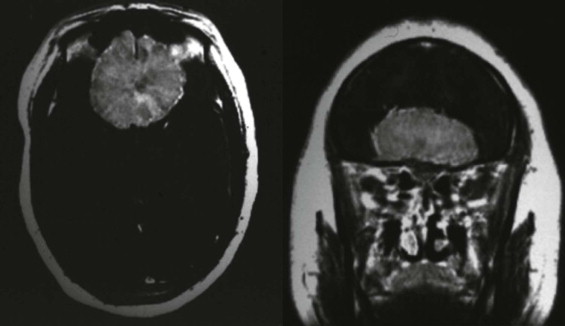
The transfrontal approach is indicated for tumors and conditions of the anterior cranial fossa, including intracranial tumors involving the cribriform plate, paranasal sinuses, and supraorbital roofs ( Figure 49-3 ).
The most common pathologic conditions are :
- •
Meningioma
- •
Fibro-osseous lesions
- •
Traumatic loss of the cribriform plate
- •
Frontal/ethmoid mucocele
- •
Osteomas
- •
Dermoid/epidermoid tumors
- •
Neurofibroma
- •
Neural sheath tumors
- •
Pituitary adenoma
- •
Craniopharyngioma
- •
Sinonasal carcinoma
- •
Chordoma
Limitations and Contraindications
Compromised frontal soft tissue requires an alternative type of closure, which could include a rotational scalp flap or a free flap. Irradiated tissue can pose problems with healing. The vascularity of the bicoronal and pericranial flap allows coverage and closure after wide field exposure of the anterior cranial fossa.
Technique: Transfrontal Approach
Step 1:
Incision
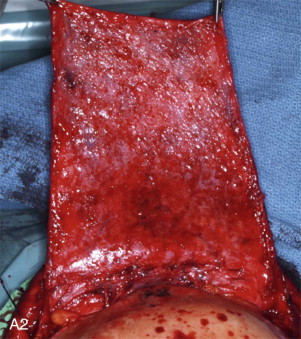
An extended bicoronal incision is used in combination with elevation of a full pericranial flap from the vertex to the supraorbital ridges ( Figure 49-4, A ).


Step 2:
Dissection
The supraorbital and supratrochlear nerves are freed as the subperiosteal dissection traverses over the supraorbital rim. A subperiosteal orbital dissection is carried out to the orbital apex.
Step 3:
Craniotomy
A bifrontal craniotomy is then performed to expose the anterior cranial fossa.
Step 4:
Dural Elevation
The frontal lobe is elevated off the anterior cranial fossa as far back as necessary, even to the sella.
Step 5:
Osteotomy
The osteotomy of the frontal bar is accomplished under direct visualization, first with vertical osteotomies of the lateral orbital rims carried through the supraorbital bar approximately 1 cm into the orbital roof. This is accomplished bilaterally ( Figure 49-4, B ).
Step 6:
Fronto-orbital Osteotomy
A reciprocating saw then is used to connect the vertical incisions traversing the frontal region at the level of the nasion. The reciprocating saw passes through the frontal sinus, which is obliterated as part of this procedure. The supraorbital bar is lifted off and placed in a saline sponge until reinsertion.
Step 7:
Cranialization
Cranialization of the frontal sinus is then performed. The posterior wall of the frontal sinus is removed using a combination of rongeurs and small bone burs. The sinus membrane is removed, and the nasal frontal ducts are imbricated, sutured primarily, or obliterated with thrombin Gelfoam sponges with tissue glue in preparation for pericranial flap closure ( Figure 49-4, C ).
Step 8:
Flap Insertion
After the interventional surgical procedure has been carried out, the pericranial flap is inserted under the supraorbital bar over the orbital roofs and attached to stable dura with 4-0 nylon sutures. If the supraorbital bar is not removed, the flap is brought over the bar. Tissue glue also can be used to aid in the stabilization of the pericranial flap. If pericranium is not available, fascia lata, temporalis muscle, or bovine pericardium can be used for barrier separation.
Step 9:
Bone Grafting
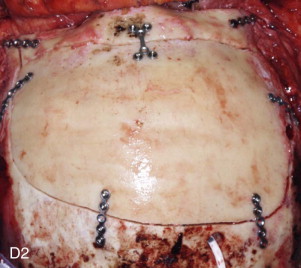
Grafting of defects of the supraorbital roof is suggested to prevent pulsatile proptosis should the orbital roofs have to be removed. The supraorbital bar is then brought back to the surgical site and stabilized with small plates. The bifrontal craniotomy bone flap is reinserted and secured with plates ( Figure 49-4, D ).
Step 10:
Closure
The bicoronal incision is closed in two layers and Jackson Pratt drains are inserted for 3 days.
Avoidance and Management of Intraoperative Complications
- 1.
The design of the bicoronal flap and the necessity of obtaining a full pericranial flap need to be decided as part of the surgical planning procedure. The decision on how to deal with the nasofrontal ducts and the frontal sinus should be made in advance. Sealing the cribriform plate from the intranasal contents is the major consideration in the transfrontal approach. Fascia lata or bovine pericardium can be used if autologous tissue is unavailable.
- 2.
Selective preoperative embolization of the tumor may be used.
- 3.
Evoked potential monitoring is used to monitor intraoperative nerve function.
Postoperative Considerations
- •
Anosmia
- •
Cerebrospinal fluid (CSF) rhinorrhea (a lumbar CSF drain may be required)
- •
Meningitis
- •
Infection
- •
Loss of bone
- •
Cosmetic defect
- •
Antibiotics are used before and after surgery.
- •
Neural deficits can occur, depending on the tumor’s location.
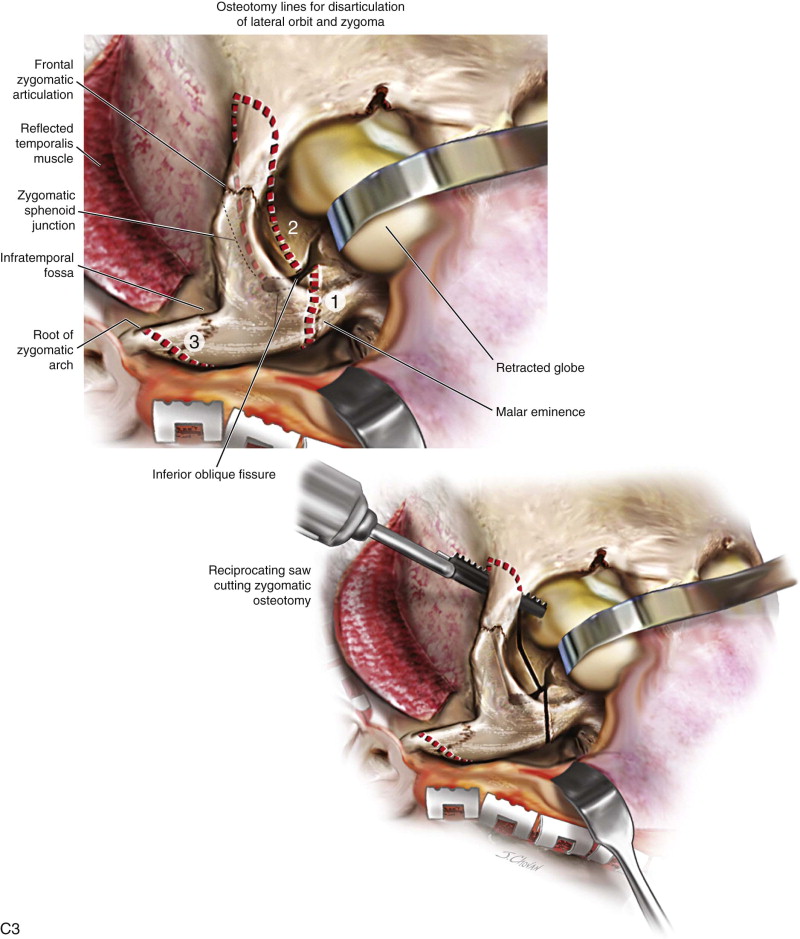
Orbital/Zygomatic Approach: Access to the Orbit, Infratemporal Fossa, Pterygoid Space, and Middle Cranial Fossa
Armamentarium
History of the Procedure
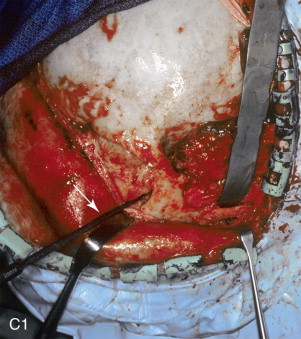
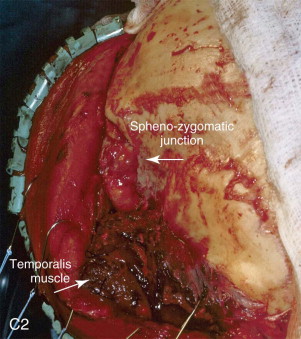
The orbital/zygomatic osteotomy is a versatile procedure that has been used for decompression of orbital proptosis and access to the infratemporal fossa. The disarticulation of the lateral orbit and zygoma replicates a fracture of the zygomaticomaxillary complex and is familiar to the maxillofacial surgeon. This procedure maintains the origin of the masseter muscle rather than using en bloc removal of the zygomatic complex.
Indications for the Use of the Procedure
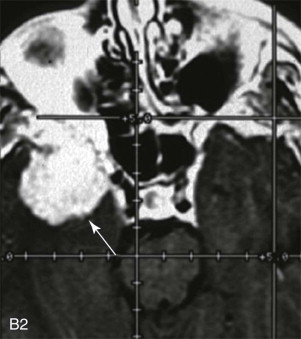
Wide field exposure is beneficial for tumors of the infratemporal fossa and orbit. Also, when combined with a frontal temporal craniotomy, it allows minimal retraction of the temporal lobe for conditions of the floor of the middle cranial fossa and sphenoid wing ( Figure 49-5, A, B ).




The most common pathologic conditions are :
- •
Meningioma
- •
Pituitary tumors
- •
Craniopharyngioma
- •
Chondrosarcoma
- •
Endochondroma
- •
Cavernous sinus pathology
- •
Cholesteatoma
- •
Temporal bone tumors
Limitations and Contraindications
Previous radiation therapy or compromised tissue may be contraindications to this procedure.
Technique: Orbital/Zygomatic Osteotomy
Step 1:
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


