Many scientific and artistic principles considered collectively are useful in creating a beautiful smile. The evaluation and analysis of the face, lips, gingival tissues and teeth are all considered in this process. Recognizing the ideal as a goal provides a direction for diagnosis and treatment planning for smile rejuvenation. This article focuses on the dental and dental–facial composition involved in smile design. Basic facial esthetics are reviewed as a guideline for facial analysis.
Smile design refers to the many scientific and artistic principles that considered collectively can create a beautiful smile. These principles are established through data collected from patients, diagnostic models, dental research, scientific measurements, and basic artistic concepts of beauty. From the patient’s perspective, beauty measures that individual’s perception of beauty as noted in the saying: “Beauty is in the eye of the beholder.” That perception of beauty may also be influenced by cultural, ethnic, or racial concepts of beauty and may vary from the standards established in the North American dental community.
When planning treatment for esthetic cases, smile design cannot be isolated from a comprehensive approach to patient care. Achieving a successful, healthy, and functional result requires an understanding of the interrelationship among all the supporting oral structures, including the muscles, bones, joints, gingival tissues, and occlusion. Gaining this understanding requires collecting all the data necessary to properly evaluate all the structures of the oral complex.
A comprehensive dental examination should include dental radiographs, mounted diagnostic models, photographic records, and a thorough clinical examination and patient interview. The clinical examination should include a smile analysis and the evaluation of the teeth, temporomandibular joints, occlusion, existing restorations, periodontal tissues, and other soft tissues of the oral cavity.
In addition to the esthetics, the function component of the anterior teeth must be considered in treatment planning. Anterior guidance in harmony with healthy joint positions is key in establishing a stable occlusal scheme. The strategic players in anterior guidance are the maxillary cuspids. A cuspid-protected occlusion helps improve the longevity of the occlusion, anterior teeth, and aesthetic restorations. It also protects the periodontium by directing the occlusal forces along the long axis of the teeth. Guiding the function to eliminate lateral and occlusal interferences helps prevent fremetus and potential joint issues resulting from traumatic occlusion.
The principles of smile design require an integration of esthetic concepts that harmonize facial esthetics with the dental facial composition and the dental composition. The dental facial composition includes the lips and the smile as they relate to the face. The dental composition relates more specifically to the size, shape, and positions of the teeth and their relationship to the alveolar bone and gingival tissues. Therefore, smile design includes an evaluation and analysis of both the hard and soft tissues of the face and smile ( Appendix 1 ).
This article focuses on the dental and dental–facial composition involved in smile design. Only basic facial esthetics are reviewed as a guideline for facial analysis. Analyzing, evaluating, and treating patients for the purpose of smile design often involve a multidiscipline approach to treatment. Specialty treatment for achieving an ideal smile can include orthodontics; orthognathic surgery; periodontal therapy, including soft tissue repositioning and bone recontouring; cosmetic dentistry; and plastic surgery. This esthetic approach to patient care produces the best dental and dental–facial beauty.
Facial beauty is based on standard esthetic principles that involve the proper alignment, symmetry, and proportions of the face. The basic shape of the face is derived from the scaffolding matrix comprised of the facial bones that form the skull and jaw as well as of the cartilage and soft tissues that overlay this framework.
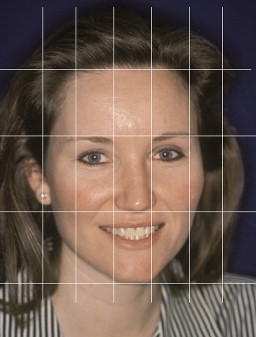
Facial features in smile design include facial height, facial shape, facial profile, gender, and age. In classical terms, the face height is divided into three equal thirds: from forehead to brow line, from brow line to the base of the nose, and from the base of the nose to the base of the chin. The width of the face is typically the width of five “eyes” ( Fig. 1 ) . As viewed from the frontal position, the four basic facial shapes recognized in the Trubyte denture tooth mold selection guide are square, tapering, square tapering, and ovoid. Lateral facial profiles can be straight, convex, or concave. A cephalometric analysis of the head in frontal and lateral views is useful in determining bony relationships of the face and the mandible, and their relationship to the teeth in the alveolar bone. The facial features related to gender and age involve the soft tissues and include the texture, complexion, and tissue integrity of the epithelial tissues.
Facial features that have a particularly important impact on the dental–facial composition are those that relate the interpupillary plane with the commisure line and the occlusal plane . The interpupillary line should be parallel with the horizon line and perpendicular to the midline of the face. In addition, the interpupillary line should be parallel with the commisure line and occlusal plane .
Lip analysis is another important soft tissue feature helpful in evaluating the dental–facial composition and establishing a smile design. The lips play an important role in that they create the boundaries of the smile design’s influence. Understanding lip morphology and lip mobility can often be helpful in meeting patients’ expectations and determining the criteria for success.
Genetic traits; the position of the teeth, alveolar bone, and jaws; and their relationships influence the shape of the lips. The upper lip is somewhat more arched and wider than the lower lip. Because the maxillary arch with the teeth overlaps the mandibular arch, the upper lip is the longer of the two. The lower lip, therefore, is recessed beneath the upper lip approximately 30° in relation to the upper lip when the arches are properly aligned .
There are three aspects of the lip morphology that should be considered: width, fullness, and symmetry. Wide lips make for a wide smile. In general terms, a smile that is at least half the width of the face, at that level of the face, is considered esthetic. The fullness and symmetry of the upper and lower lips should also be documented. The fullness of the lip, or lip volume, can be categorized as full, average, or thin. Lip symmetry involves the mirror image appearance of each lip when smiling.
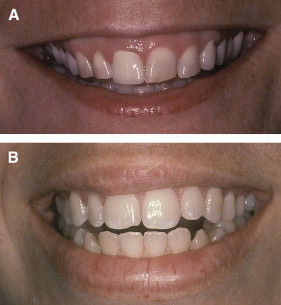
The upper and lower lips should be analyzed separately and independently of one another. Independent evaluation of the upper and lower lip is essential when analyzing both symmetry and fullness. The question should be asked: “Are the upper and lower lips symmetric on both sides of the midline and do they have the same degree of fullness?” In Fig. 2 A, the upper and lower lips are symmetric but they differ in fullness. In Fig. 2 B the upper lip is asymmetric and the lower lip is symmetric and the fullness is similar. Recognizing the etiology of lip asymmetries is helpful in determining if there is a dental solution for improvement or if plastic surgery is necessary. Sometimes both are necessary to provide the results desired by the patient.
The position of the lips in the rest position should be evaluated for lip contact as well as for the range of lip mobility when smiling. These two determinants establish how much tooth structure and gingival tissue are revealed when comparing the repose and full smile positions. Evaluating this dental–facial feature can be helpful in analyzing and determining treatment modalities necessary to improve the smile. Lip evaluation is also useful when considering the patient’s expectation and, more importantly, for revealing tooth and tissue asymmetries or defects.
When smiling, the inferior border of the upper lip as it relates to the teeth and gingival tissues is called the lip line. An average lip line exposes the maxillary teeth and only the interdental papillae. A high lip line exposes the teeth in full display as well as gingival tissues above the gingival margins. A low lip line displays no gingival tissues when smiling. In most cases, the lip line is acceptable if it is within a range of 2 mm apical to the height of the gingiva on the maxillary centrals .
In cases where there is a high lip line and an excessive gingival display exists, an unwanted “gummy smile” becomes evident. Several corrective options are available, depending on conditions and patient limitations. With cephalometric analysis, vertical maxillary excess can be determined. Orthodontics and orthognathic surgery to impact the maxilla are ideal when these conditions are confirmed as skeletal displasias in nature.
In other cases where apparent diminished tooth size in combination with a high lip line creates a gummy smile, corrective periodontal procedures are an option . This involves cases where altered passive eruption makes a normal-sized tooth appear small. Altered passive eruption occurs when the pellicle does not completely recede to the cementoenamel junction . As a result, the tooth appears short because the gingival portion of the enamel, which is usually exposed, remains covered with gingival tissues.
Cosmetic crown lengthening to expose the covered enamel can improve normal tooth height and tooth proportions. This can produce a more pleasing emergence profile of the tooth. These procedures can also be helpful in creating symmetry, positive radicular architecture, and proper zenith points of the gingival margins. Many times when exostosies exists, recontouring the alveolar bone is also necessary to recreate and define normal architecture and prevent a ledging appearance of the gingival tissues.
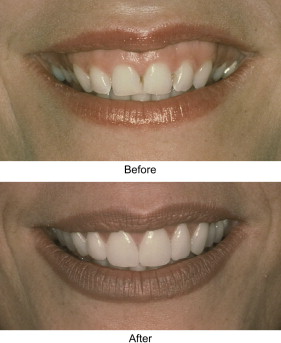
The frenum attachment can also affect the upper-lip shape and the amount of tooth exposure. In such cases, especially where the attachment is broad, a frenectomy that is dissected out from origin to insertion, removing the elastic fibers, can also free up the lip for normal lip movement. This can also be useful when a redundant flap of tissue, termed by this author as a “lip curtain” ( Fig. 3 ), is visible hanging beneath the upper lip when smiling. These procedures, used in combination with cosmetic dental procedures, can reduce gummy smiles and produce a more esthetic smile ( Fig. 4 ).

The incisal display refers to the amount of visible tooth displayed when the lips and lower jaw are in the rest position. The average incisal display of the maxillary centrals for males is 1.91 mm and the average for females is 3.40 mm . With age, the amount of incisal display of the maxillary centrals diminishes and the amount of incisal display of the mandibular centrals increases . Therefore, the amount of incisal display is an important factor in a youthful smile.
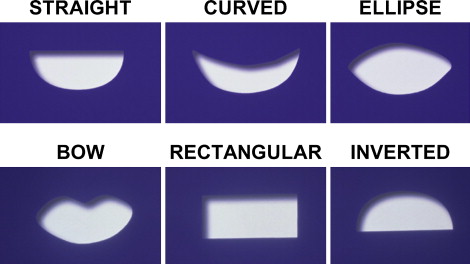
The inferior border of the upper lip and the superior border of the lower lip form an outline of the space that is revealed when smiling. The curvature of the lips as well as the prevalence of the shapes formed by the lips has been noted in texts . The space that includes the teeth and tissues is called the smile zone . There are six basic smile-zone shapes: straight, curved, elliptical, bow-shaped, rectangular, and inverted ( Fig. 5 ). The first three shapes are the most common. Identifying these shapes is helpful in analyzing the smile.
A feature of smile design that is often overlooked yet very significant is the health, symmetry, and architecture of the gingival tissues. These tissues frame the teeth and add to the symmetry of the smile. The health and subsequent color and texture of these gingival tissues are paramount for long-term success and the esthetic value of the treatment.
Healthy gingival tissues are pale pink and can vary in degree of vascularity, epithelial kertinization, and pigmentation, and in the thickness of the epithelium. The papillary contour should be pointed and should fill the interdental spaces to the contact point. An unfilled interdental space creates an unwanted black interdental triangle in the gingival embrasure and makes a smile less attractive ( Fig. 6 ). Managing the soft tissues in this area improves the smile when these tissues are revealed. The architecture has a positive radicular shape forming a scalloped appearance that is symmetric on both sides of the midline. The marginal contour of the gingival should be sloped coronally to the end in a thin edge. The texture of the tissues should be stippled (orange-peel–like appearance) in most cases. The stippling may be fine or coarse and the degree of stippling varies. In younger females, the tissue is more finely textured and has a finer stippling when compared with that of males. The tissue should be firm in consistency and the attached part should be firmly anchored to the teeth and underlying alveolar bone. A normal, healthy gingival sulcus should not exceed 3 mm in depth .

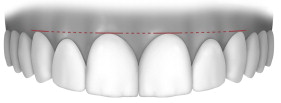
The gingival contours should be symmetric and the marginal gingival tissues of the maxillary anterior teeth should be located along a horizontal line extending from cuspid to cuspid. Ideally, the laterals reach slightly short of that line ( Fig. 7 ) . It is also acceptable, although not ideal, to have the gingival height of all six anteriors equal in gingival height on the same plane ( Fig. 8 ). In such cases, however, the smile may appear too uniform to be esthetically pleasing. A gingival height of the laterals that is more apical to the centrals and cuspids is considered unattractive ( Fig. 9 ).