Introduction
The objective of this investigation was to compare the amount of apical root resorption in nonextraction treatment of Class II malocclusions with and without Class II elastics.
Methods
A sample of 54 patients with Class II Division 1 malocclusion, retrospectively selected, was divided into 2 groups. The elastic group consisted of 27 patients who were exclusively treated with fixed appliances associated with elastics, and the headgear group consisted of 27 patients treated with fixed appliances and extraoral headgear. The groups were matched regarding initial age, treatment time, amount of overjet, initial malocclusion severity, final occlusal status, and severity of Class II molar relationship. Posttreatment periapical radiographs of the maxillary and mandibular central and lateral incisors were used to evaluate root resorption. The amounts of resorption in the groups were compared with Mann-Whitney U tests.
Results
There was no statistically significant difference in the amounts of root resorption between the elastic and the headgear groups.
Conclusion
Nonextraction treatment of Class II malocclusions with Class II elastics associated with fixed appliances causes similar root resorption as treatment with extraoral headgear and fixed appliances. Apical root resorption was predominantly mild and similar in the 2 groups.
Highlights
- •
Intermaxillary elastics, especially Class II elastics, might cause root resorption.
- •
We evaluated root resorption after Class II malocclusion correction with elastics.
- •
Elastics plus fixed appliances caused similar root resorption as other treatments.
A Class II malocclusion is a major reason that patients seek orthodontic treatment, and it requires different types of treatment when severity of the anteroposterior discrepancy, age, and patient compliance are considered. There are a number of orthodontic appliances and accessories to treat a Class II malocclusion and Class II elastics are among them.
Tucker was one of the first to use rubber in his appliances, such as rubber bands or tubes for tooth movement. The use of intermaxillary elastics has been a standard procedure in the correction of Class II malocclusions since the early days of orthodontic treatment, when their use was pioneered by Calvin S. Case of Chicago and Henry A. Baker of Boston in the 1890s.
It is well documented in the literature that although intermaxillary elastics are effective in correcting the anteroposterior relationship of the dentition, undesirable side effects may occur. Many authors have noted adverse results caused by the vertical force vector that is inherent with intermaxillary elastics. It has been stated that this vertical force may extrude the maxillary incisors and mandibular molars, causing clockwise rotation of the occlusal plane and the mandible when Class II elastics are used.
There are no evidence-based studies that definitively establish the optimum force for Class II elastics. Some studies have suggested that the long-term jiggling force caused by the intermittent use of elastics might increase the prevalence of incisor root resorption, and indicated that Class II elastics are a significant risk factor.
Root resorption, particularly in the anterior teeth, is frequently reported in orthodontic treatment and has been recognized by clinical investigators in daily practice since Ketcham first reported it in 1927.
The association of root resorption with orthodontic therapy is complex, and several treatment risk factors were reported, alone or in combination. Amount of apical displacement, type of malocclusion, orthodontic movement type, and treatment duration are directly associated with root resorption. When mechanical factors are mentioned, the type and the amount of orthodontic force were considered the main causes of apical resorption. Consequently, treatment of a Class II malocclusion, whether nonextraction or with 2 or 4 premolar extractions, is also likely to cause some root resorption, independently of the appliances or mechanics used.
However, the amount of root resorption from the use of Class II elastics in Class II malocclusion correction has not been evaluated. Therefore, the purpose of this investigation was to test the following null hypothesis: apical root resorption in nonextraction treatment of Class II malocclusions with or without Class II elastics is similar.
Material and methods
This study was approved by the ethics research committee of Bauru Dental School, University of São Paulo, Bauru, São Paulo, Brazil, and all subjects signed informed consent.
The sample size was calculated based on an alpha significance level of 5% and a beta of 20% to achieve 80% power to detect a mean difference of 0.32 with a standard deviation of 0.39 in the degree of root resorption. The results showed that a minimum of 25 patients were needed for each group.
Therefore, a sample of 54 Class II Division 1 malocclusion patients who were treated without extractions was retrospectively selected from the files of the orthodontic department at Bauru Dental School, University of São Paulo, Bauru, São Paulo, Brazil. The sample was divided into 2 groups. The elastic group (EG) consisted of 27 patients (11 boys, 16 girls) treated with fixed appliances associated with Class II elastics, and the headgear group (HG) consisted of 27 patients (12 boys, 15 girls) treated with fixed appliances and extraoral headgear.
Patients were selected according to the following inclusion criteria: Class II Division 1 malocclusion with a minimum of a half Class II molar relationship, treatment completed with no permanent teeth extracted (excluding third molars), good occlusal finishing, and good-quality pretreatment and posttreatment periapical radiographs. Patients with endodontic treatment; history of trauma, nail biting, and other habits; impacted canines or dental anomalies of number; apical root resorption; and incomplete orthodontic records were excluded. No patient had been retreated or subjected to palatal expansion.
The common mechanics in the 2 groups consisted of standard fixed edgewise or Roth preadjusted appliances with 0.022 × 0.028-in slots and a usual wire sequence characterized by an initial 0.015-in twist-flex or a 0.016-in nickel-titanium alloy, followed by 0.016, 0.018, 0.020, and 0.019 × 0.025 or 0.018 × 0.025-in stainless steel archwires. Deep overbites were corrected by reversed and accentuated curve of Spee.
In the EG, the Class II anteroposterior discrepancy was corrected with Class II elastics on both sides for at least 6 months, 15 to 18 hours a day, with a mean force of 200 g, measured with a tension gauge ( Fig 1 ). The elastics were used more on 1 side than the other, when necessary.
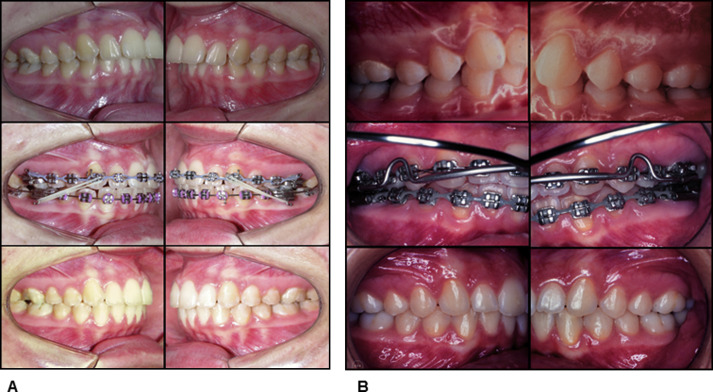
In the HG, extraoral headgear was used to distalize the maxillary teeth or restrict maxillary forward displacement to correct the Class II anteroposterior discrepancy ( Fig 1 ). Treatment times were calculated from the patients’ records.
On the pretreatment and posttreatment dental study casts, the initial malocclusion severity of the groups was evaluated with the Peer Assessment Rating (PAR) index, and the quality of the treatment results was obtained with the Objective Grading System (OGS), developed by the American Board of Orthodontics. The scores were blindly assigned by a previously calibrated examiner (A.N.).
The degree of root resorption during orthodontic treatment was blindly evaluated by a previously calibrated examiner (A.N.) on the posttreatment periapical radiographs of the maxillary and mandibular central and lateral incisors.
Periapical radiographs were obtained with the DABI 70 Spectro 1070X x-ray machine (Dabi Atlante, Ribeirão Preto, Brazil), set up at 70 kV, 10 mA, and exposure time of 1 second, using the long-cone paralleling technique. Ektaspeed EP 21 films (Eastman Kodak, Rochester, NY) were used, and the angles were obtained by an intraoral XCP positioner (Dentsply Rinn, Elgin, Ill).
The initial and final periapical radiographs were scanned with the Sprint Scan 35 Plus scanner (version 2.7.2; Polaroid, Cambridge, Mass), with a resolution of 675 dpi at a scale of 1:1. The initial radiographs were used as a parameter of the resorption severity during this evaluation. The images were analyzed with Photoshop software (version 6.0; Adobe Systems, San Jose, Calif) at 300% enlargement, without image quality loss.
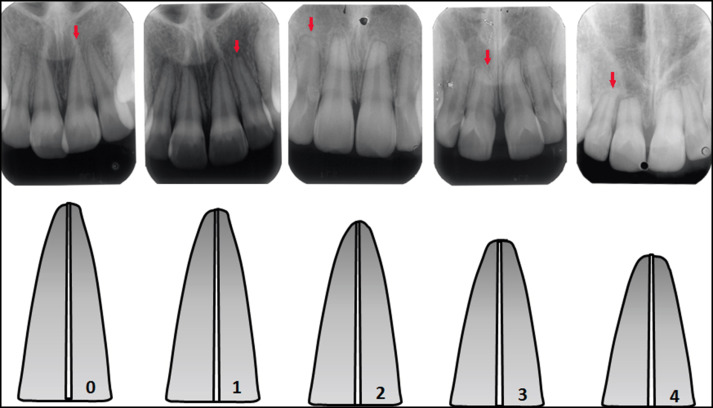
To evaluate the amount of root resorption, the score system of Malmgren et al was used. Signs of apical root resorption were recorded according to 5 scores defined from 0 to 4 ( Fig 2 ).
The reproducibility of the measurements was assessed by analyzing the difference between double evaluations of root resorption by the same examiner, taken with an interval of 30 days of all final periapical radiographs. Intraexaminer agreement was calculated with kappa statistics.
After a 30-day interval, 15 dental casts and panoramic radiographs were also randomly selected and remeasured by the same examiner. The random error was calculated according to Dahlberg’s formula (Se 2 = ∑d 2 /2n), where Se 2 is the error variance and d is the difference between 2 determinations of the same variable, and the systematic error was calculated with dependent t tests, at P <0.05.
Statistical analyses
Normal distribution of the variables was verified with Kolmogorov-Smirnov tests. All variables showed a normal distribution.
The groups were compared regarding initial age, treatment time, overjet, initial malocclusion severity (PAR), and quality of the treatment results (OGS) with t tests. Intergroup sex percentages and severity of Class II molar relationships were compared with chi-square tests. Because apical movement is correlated with root resorption, the amounts of maxillary and mandibular incisor inclination changes were compared between the groups with t tests. Maxillary and mandibular incisor inclinations were evaluated by measuring the angles between the incisors’ long axes and the NA and NB lines, respectively. Treatment changes were calculated as pretreatment measurements subtracted from posttreatment measurements.
Intergroup root resorption was compared with Mann-Whitney U tests, as an overall score for the groups and for each tooth.
Descriptive statistics were used to show the tooth distribution among the scores of root resorption according to the method of Malmgren et al.
The results were considered significant at P <0.05. The statistical analyses were performed with Statistica for Windows 10 software (StatSoft, Tulsa, Okla).
Results
Intraexaminer reproducibility of the evaluation of root resorption showed almost perfect and substantial agreement between the first and second evaluations ( Table I ).
| Tooth number ∗ | Observed agreement (%) | Kappa | Strength of agreement † |
|---|---|---|---|
| 12 | 39 (78) | 0.78 | Substantial |
| 11 | 39 (78) | 0.78 | Substantial |
| 21 | 47 (94) | 0.94 | Almost perfect |
| 22 | 41 (82) | 0.82 | Almost perfect |
| 42 | 42 (84) | 0.84 | Almost perfect |
| 41 | 50 (100) | 1.00 | Almost perfect |
| 31 | 50 (100) | 1.00 | Almost perfect |
| 32 | 49 (98) | 0.98 | Almost perfect |
∗ Fédération Dentaire Internationale tooth-numbering system.
† According to the classification suggested by Landis and Koch for kappa test results.
No statistically significant systematic errors were detected, and the random errors were within acceptable levels ( Table II ).
| Variable | First measurement Mean/SD |
Second measurement Mean/SD |
Dahlberg | P |
|---|---|---|---|---|
| Initial PAR | 8.70/3.13 | 7.80/3.49 | 1.50 | 0.193 |
| OGS | 18.80/7.10 | 18.50/3.44 | 2.82 | 0.828 |
| Overjet (mm) | 6.65/2.66 | 6.65/2.76 | 0.69 | 1.000 |
The groups were matched regarding initial age, treatment time, overjet, initial malocclusion severity (PAR), final occlusal status (OGS), sex distribution, and severity of the Class II molar relationship. However, the EG had a statistically longer treatment time than did the HG ( Table III ). Incisor inclination treatment changes were similar in the groups.
| Variable | Elastic group (n = 27) Mean/SD |
Headgear group (n = 27) Mean/SD |
P |
|---|---|---|---|
| Initial age (y) | 12.96/1.46 | 12.61/1.10 | 0.334 † |
| Treatment time (y) | 2.85/1.14 | 1.87/0.88 | 0.001 ∗ † |
| Overjet (mm) | 5.77/2.81 | 6.20/3.22 | 0.607 † |
| Initial PAR index | 10.51/3.71 | 10.44/3.45 | 0.939 † |
| OGS | 23.66/7.28 | 19.11/10.41 | 0.068 † |
| Sex | 0.783 ‡ | ||
| Male | 11 | 12 | |
| Female | 16 | 15 | |
| Severity of molar relationship | 0.402 ‡ | ||
| Complete Class II | 12 | 9 | |
| Half Class II | 15 | 18 | |
| Incisor inclination treatment changes | |||
| Mx1.NA (°) | −0.73/8.90 | 0.96/10.62 | 0.534 |
| Md1.NB (°) | 3.09/5.63 | 4.13/6.23 | 0.528 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


