Introduction
The aim of this study was to determine the reproducibility and accuracy of linear measurements on 2 types of dental models derived from cone-beam computed tomography (CBCT) scans: CBCT images, and Anatomodels (InVivoDental, San Jose, Calif); these were compared with digital models generated from dental impressions (Digimodels; Orthoproof, Nieuwegein, The Netherlands). The Digimodels were used as the reference standard.
Methods
The 3 types of digital models were made from 10 subjects. Four examiners repeated 37 linear tooth and arch measurements 10 times. Paired t tests and the intraclass correlation coefficient were performed to determine the reproducibility and accuracy of the measurements.
Results
The CBCT images showed significantly smaller intraclass correlation coefficient values and larger duplicate measurement errors compared with the corresponding values for Digimodels and Anatomodels. The average difference between measurements on CBCT images and Digimodels ranged from −0.4 to 1.65 mm, with limits of agreement values up to 1.3 mm for crown-width measurements. The average difference between Anatomodels and Digimodels ranged from −0.42 to 0.84 mm with limits of agreement values up to 1.65 mm.
Conclusions
Statistically significant differences between measurements on Digimodels and Anatomodels, and between Digimodels and CBCT images, were found. Although the mean differences might be clinically acceptable, the random errors were relatively large compared with corresponding measurements reported in the literature for both Anatomodels and CBCT images, and might be clinically important. Therefore, with the CBCT settings used in this study, measurements made directly on CBCT images and Anatomodels are not as accurate as measurements on Digimodels.
Highlights
- •
Measurements on Digimodels, Anatomodels, and CBCT scans were significantly statistically different.
- •
Measurements on Anatomodels and Digimodels were more reproducible than those on CBCT scans.
- •
Measurements on Digimodels were the most accurate.
In orthodontics, study model analysis is an essential part of the diagnosis, treatment planning, and evaluation of treatment progress. When digitalization was introduced in the orthodontic world, digital models became available to replace traditional plaster casts. The most frequently used method to obtain digital dental models is to digitize plaster models or dental impressions. The technology used to generate digital models from dental models or impressions varies considerably. Orthocad (Cadent, Carlstadt, NJ) uses “destructive scanning” with multiple scans of the plaster model cut in thin slices. Emodels (GeoDigm, Falcon Heights, Minn) scans the surface of a complete plaster model. Impressions can also be scanned directly using cone-beam computed tomography (CBCT) technology (Digimodels; Orthoproof, Nieuwegein, The Netherlands).
Digitized plaster models or digital models derived from dental impressions have been shown to be a valid tool for undertaking simple diagnostic measurements such as tooth size, arch width, overjet, overbite, arch length, and Bolton ratio. In a systematic review, Fleming et al found that overall, the mean differences between linear measurements on plaster and digital models were small (0.04-0.4 mm).
Digital dental models provide several advantages over plaster models. Digital models can be stored electronically; this reduces storage space and the risk of damage. Furthermore, digital models can be shared easily over a network. A copy of the digital model can be secured at a second site for minimal or no costs. However, computer failure might mean that the models are temporarily or forever inaccessible.
Now, study model analysis can also be performed directly on radiographs, such as CBCT scans, without the need for impressions. Study model analysis can be done directly on the radiograph of the head with dedicated software. For example, Anatomage software (InVivoDental, San José, Calif) can be used to measure the dentition on a CBCT image. The files of a CBCT image can also be sent by e-mail to InVivoDental for segmentation of the dentition to produce digital dental models (Anatomodels). Study model analysis can be done directly on these Anatomodels using the Anatomage measuring tools. The accuracy of linear measurements of the dentition on these Anatomodels for orthodontic purposes has been reported in 4 articles. According to these publications, the accuracy of measurements on Anatomodels is related to the voxel size and spatial resolution of the CBCT images. Reduction of the spatial resolution can result in a lower-quality image, more noise and artifacts, and less anatomic information. Spatial resolution is lower at shorter scanning times and larger voxel sizes. Only in 1 study, a shorter scanning time, lower kilovoltage (129 kV), lower milliamperage (47.74 mA), and a voxel size of 0.4 mm were used. In all other studies, a smaller voxel size (0.3 mm) and longer scanning times were applied. A longer scanning time improves the spatial resolution but also increases the radiation dose.
To our knowledge, no study has compared the accuracy of measurements directly performed on CBCT images (without segmentation of the dentition) with Anatomodels and Digimodels, and only 1 article used CBCT scans with a voxel size of 0.4 mm and shorter scanning time for measuring the dentition. Therefore, the aim of this study was to examine the reproducibility and accuracy of linear measurements on CBCT images and Anatomodels obtained from CBCT images with a relatively large voxel size of 0.4 mm and a relatively short scanning time compared with the reference measurements on Digimodels.
Material and methods
From the archives of the Department of Orthodontics and Craniofacial Biology of the Radboud University Medical Centre in The Netherlands, pretreatment records were selected of patients who met the following inclusion criteria: (1) impressions to fabricate digital models and a CBCT image obtained on the same day; (2) permanent dentition from left first molar to right first molar in both arches; (3) normal dental crown morphology; (4) no features that would influence crown morphology such as restorations, caries, attrition, or fracture; (5) good-quality digital dental models without irregularities; and (6) the measurements were not compromised by streaking artifacts on the CBCT radiographs, caused by metal restorations or fixed appliances, because these patients had no metal restorations or orthodontic appliances. Twenty-four patients met these inclusion criteria. Ten patients from this group were randomly selected for this study.
The CBCT scans were retrieved from the CBCT database of patients who had combined surgical and orthodontic treatment at the Radboud University Medical Centre. These extended-height scans were used for 3-dimensional planning for the orthognathic surgery. All patients signed the informed consent form for this treatment, including the CBCT documentation. The following settings where used for the i-CAT 3D Imaging System (Imaging Sciences International, Hatfield, Pa): 129 kV, 47.74 mA, 40 seconds with a resolution of 0.4 mm/voxel, and a field of view of 17 cm in diameter and 22 cm in height.
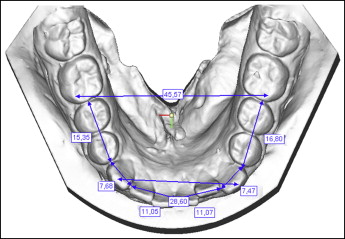
For each patient, 3 types of dental models were analyzed: Digimodels, CBCT images, and Anatomodels. The Digimodels were used as the reference standard. To process the Digimodels ( Fig 1 ), alginate dental impressions (Orthotrace; Cavex Holland BV, Haarlem, The Netherlands) were sent to the OrthoProof company on the same day as the impressions were taken. Within 24 hours, the impressions were scanned with a computed tomography scanner with a voxel size of 0.15 mm (Hytec, Los Alamos, NM). Subsequently, the scanned data were used to fabricate digital models. These Digimodels were imported through the Internet from the OrthoProof Web server into the patient management system at the Radboud University Medical Centre. Study model analysis of the digital dental models was conducted with the Digimodels software.
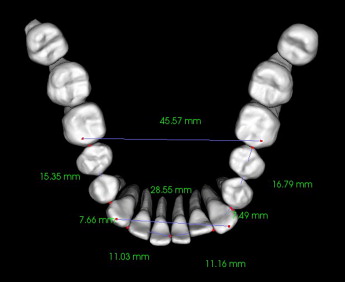
Alternatively, study model analysis can be carried out directly on the digital image of the dentition on the CBCT image using dedicated software. The DICOM files of the CBCT images were sent by e-mail to the Anatomage company for segmentation of the dentition from the CBCT images to process the digital dental models, which are called Anatomodels. The company uses automatic thresholding logarithms for the segmentation process and does not share information on this rendering process.
Four dental students were trained and calibrated to perform the measurements on the 2 digital models and the CBCT image of each patient. The definitions of the 37 measurements used in this study are given in Table I . Figures 1 to 3 show examples of the measurements on the 3 different models. The measurements on the Digimodels were carried out with the Digimodel software (version 2.2.1; Orthoproof) on a 15-in monitor with a resolution of 1280 × 800 pixels and 32-bit color-screen setting.
| Measurement | Definition |
|---|---|
| Mesiodistal width of the crowns of incisors, canines, and premolars (maxilla and mandible) | Distance between the distal and mesial contact points of incisors, canines, premolars, respectively (mm) (20 distances) |
| Intermolar distance in maxilla and mandible | Distance between the top of the mesiobuccal cusps of the first permanent molars (mm) (2 distances) |
| Intercanine distance in maxilla and mandible | Distance between the cusps of the canines (mm) (2 distances) |
| Interincisal distance | Distance between the incisal edges of the maxillary and mandibular incisors ( mm) measured on a central point of the incisal edge of teeth 11 and 41 |
| Segment A | Distal contact point of tooth 15 to the mesial contact point of 14 |
| Segment B | Mesial contact point of tooth 14 to the distal contact point of 12 |
| Segment C | Distal contact point of tooth 12 to the mesial contact point of 11 |
| Segment D | Mesial contact point of tooth 11 to the distal contact point of 22 |
| Segment E | Distal contact point of tooth 22 to the mesial contact point of 24 |
| Segment F | Mesial contact point of tooth 24 to the distal contact point of 25 |
| Segment G | Distal contact point of tooth 35 to the mesial contact point of 34 |
| Segment H | Mesial contact point of tooth 34 to the distal contact point of 32 |
| Segment I | Distal contact point of tooth 32 to the mesial contact point of 31 |
| Segment J | Mesial contact point of tooth 31 to the distal contact point of 42 |
| Segment K | Distal contact point of tooth 42 to the mesial contact point of 41 |
| Segment L | Mesial contact point of tooth 44 to the distal contact point of 45 |
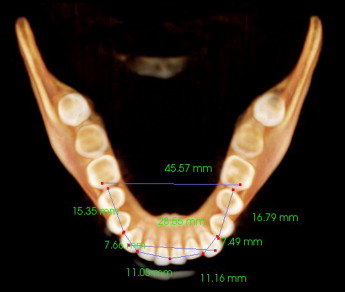
The measurements on the CBCT images and Anatomodels were carried out with the Anatomage measuring program on a 20-in computer monitor with the same resolution and color depth setting as the 15-in monitor. The measurements on the CBCT images were taken on the 3-dimensional rendered images. Enlargement, clipping, and rotation of the images to facilitate the measurements were routinely performed. There was no time limit for performing the measurements. All measurements were repeated 10 times by the 4 observers; this means that each of the 37 measurements was repeated 40 times. There was an interval of at least 2 weeks between the series of measurements.
Statistical analysis
Interobserver reliability was assessed by calculating the intraclass correlation coefficient (ICC). Intraobserver reliability was assessed by the individual mean standard deviations of the measurements for the 4 observers. An ICC of 0.90 or higher is considered excellent, between 0.75 and 0.90 is good, and between 0.50 and 0.75 is moderate. An ICC less than 0.50 is considered to be poor. Statistical significance was set at P <0.05.
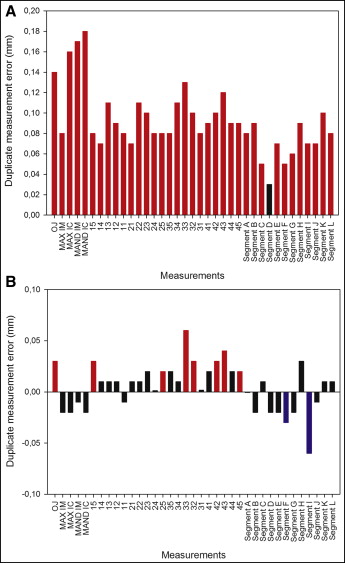
The reproducibility of the measurements was assessed by comparing the duplicate measurement errors of the 3 study models.
Means and standard deviations were calculated for all variables, and limits of agreement values were calculated for all crown-width measurements to assess the accuracy of the measurements on the 3 study models. The differences between the means of the variables on the Digimodels, CBCT images, and Anatomodels for the 4 observers were calculated. The paired t test was used to evaluate the differences between the mean values of each variable. Statistical analysis was performed with the Statistical Package for Social Sciences software (version 18.2; SPSS, Chicago, Ill).
Results
The interobserver reliability values were determined for all 37 variables of the 2 models and the CBCT images separately. The mean ICC values were 0.88 (range, 0.62-0.99) for measurements on the Digimodels, 0.76 (range, 0.20-0.98) for the CBCT images, and 0.92 (range, 0.76-0.99) for Anatomodels. The ICC values for the Digimodels were considered good or excellent for 33 of the 37 variables (higher than 0.75) and moderate for the other 4 measurements. For the CBCT images, the ICC values were good for 22 measurements, moderate for 13 measurements (between 0.5 and 0.75), and poor for 2 measurements (<0.5). Especially, the intercanine and intermolar distances in the mandible had low ICC values on the CBCT images. On the Anatomodels, the ICC values for all measurements were above 0.75.
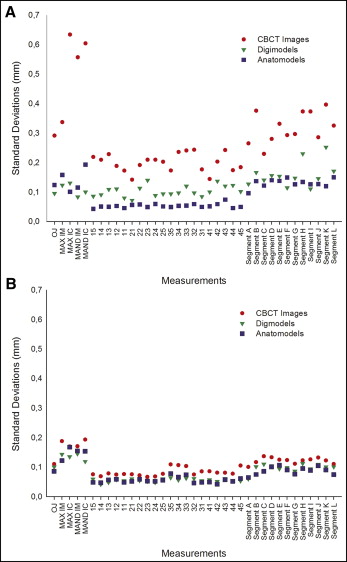
To test the intraobserver reliability of the 4 observers, the individual standard deviations of the measurements were determined. The intraobserver reliability of the observers with the largest and the smallest standard deviations in measurements are shown in Figure 4 . All 4 observers showed larger standard deviations for the CBCT images compared with the measurements on the Digimodels and the Anatomodels. The intraobserver reliability values for measurements on these models were comparable.
When comparing the duplicate measurement errors for Digimodels and CBCT images, 36 of the 37 duplicate measurement errors were significantly larger on the CBCT images.
Ten statistically significant and different duplicate measurement errors were found between the Anatomodels and the Digimodels: 8 measurements had larger duplicate measurement errors on the Anatomodels, and 2 measurements of segments had smaller duplicate measurement errors on the Anatomodels. Differences between the duplicate measurement errors of the 3 digital models are presented in Figure 5 .
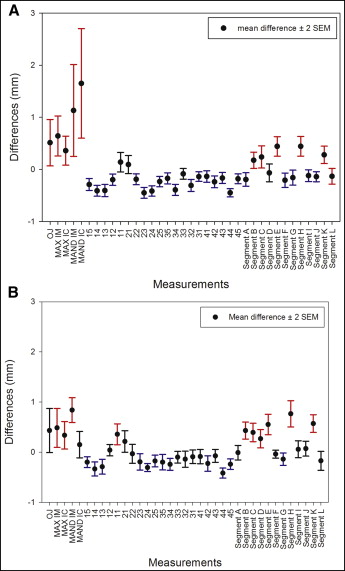
The mean values of the variables measured on Digimodels, CBCT images, and Anatomodels were compared. Statistically significant differences between measurements on the CBCT images models and the Digimodels ( P values <0.05) were found in 32 of the 37 measurements. Of these 32 variables, 24 variables measured on the CBCT images were smaller and 8 were larger compared with the measurements on the Digimodels. The mean difference for crown width between these models ranged from 0.14 to −0.45 mm. The corresponding lower and upper limits of the 95% confidence interval of the difference were −0.55 and 0.33 mm, respectively ( Fig 6 , A ; Table II ). The mean difference in measurements for the transversal, segmental, and interincisal distances ranged from −0.2 to 1.65 mm. The corresponding lower and upper limits of the 95% confidence interval of the difference were −0.35 and 2.71 mm, respectively ( Fig 6 , A ). All statistically significant crown-width measurements were smaller on the CBCT images. All significant intermolar, intercanine, and interincisal distances were larger on the CBCT images ( Fig 6 , A ). Statistically significant differences between the Digimodels and the Anatomodels were found for 22 measurements. Twelve measurements on Anatomodels were smaller, and 10 measurements were larger. The mean difference in crown widths between Digimodels and Anatomodels ranged from 0.36 to −0.42 mm. The corresponding lower and upper limits of the 95% confidence interval of the difference were −0.52 and 0.57 mm, respectively ( Fig 6 , B ; Table II ). The mean difference for measurements of the transversal, segmental, and interincisal distances on these models had a range of −0.17 to 0.84 mm. The corresponding lower and upper limits of the 95% confidence interval of the difference were −0.36 and 1.09 mm, respectively ( Fig 6 , B ). Compared with the measurements on the Digimodels, all significant intermolar, intercanine, and interincisal distances were larger on the Anatomodels. All significant crown-width measurements on the Anatomodels were smaller compared with the same measurements on the Digimodels, except for the maxillary right central incisor.
| Mean difference | Limits of agreement | Duplicate measurement error | |||||||
|---|---|---|---|---|---|---|---|---|---|
| P | Difference | 95% CI of the difference | P | Difference | 95% CI of the difference | ||||
| Lower | Upper | Lower | Upper | ||||||
| Crown-width measurements: Anatomodels-Digimodels | |||||||||
| 15 | 0.001 | −0.20 | −0.31 | −0.09 | −0.86…0.46 | 0.003 | 0.03 | 0.01 | 0.05 |
| 14 | 0.001 | −0.33 | −0.47 | −0.19 | −1.20…0.53 | 0.422 | 0.01 | −0.01 | 0.03 |
| 13 | 0.001 | −0.29 | −0.44 | −0.14 | −1.21…0.63 | 0.240 | 0.01 | −0.01 | 0.04 |
| 12 | 0.473 | 0.04 | −0.07 | 0.16 | −0.67…0.75 | 0.291 | 0.01 | −0.01 | 0.04 |
| 11 | 0.001 | 0.36 | 0.15 | 0.57 | −0.93…1.65 | 0.723 | −0.01 | −0.05 | 0.04 |
| 21 | 0.052 | 0.21 | −0.02 | 0.43 | −1.11…1.54 | 0.278 | 0.01 | −0.01 | 0.03 |
| 22 | 0.742 | −0.03 | −0.22 | 0.16 | −1.19…1.13 | 0.365 | 0.01 | −0.01 | 0.03 |
| 23 | 0.024 | −0.19 | −0.36 | −0.03 | −1.21…0.82 | 0.069 | 0.02 | 0.001 | 0.05 |
| 24 | 0.001 | −0.31 | −0.39 | −0.23 | −0.8…0.19 | 0.872 | 0.001 | −0.02 | 0.01 |
| 25 | 0.004 | −0.17 | −0.29 | −0.06 | −0.89…0.54 | 0.037 | 0.02 | 0.001 | 0.04 |
| 35 | 0.015 | −0.20 | −0.36 | −0.04 | −1.16…0.77 | 0.114 | 0.02 | 0.001 | 0.04 |
| 34 | 0.001 | −0.24 | −0.36 | −0.12 | −0.97…0.49 | 0.369 | 0.01 | −0.01 | 0.03 |
| 33 | 0.093 | −0.10 | −0.22 | 0.02 | −0.82…0.62 | 0.001 | 0.06 | 0.03 | 0.08 |
| 32 | 0.093 | −0.14 | −0.3 | 0.02 | −1.14…0.86 | 0.002 | 0.03 | 0.01 | 0.06 |
| 31 | 0.186 | −0.09 | −0.23 | 0.05 | −0.93…0.74 | 0.867 | 0.001 | −0.02 | 0.02 |
| 41 | 0.226 | −0.09 | −0.23 | 0.06 | −0.96…0.79 | 0.116 | 0.02 | 0.001 | 0.04 |
| 42 | 0.006 | −0.22 | −0.38 | −0.07 | −1.18…0.73 | 0.008 | 0.03 | 0.01 | 0.06 |
| 43 | 0.268 | −0.07 | −0.20 | 0.06 | −0.87…0.72 | 0.003 | 0.04 | 0.01 | 0.06 |
| 44 | 0.001 | −0.42 | −0.52 | −0.31 | −1.04…0.2 | 0.241 | 0.02 | −0.01 | 0.04 |
| 45 | 0.001 | −0.24 | −0.35 | −0.13 | −0.90…0.42 | 0.025 | 0.02 | 0.001 | 0.04 |
| Crown-width measurements: CBCT images-Digimodels | |||||||||
| 15 | 0.001 | −0.29 | −0.40 | −0.18 | −0.99…0.41 | 0.001 | 0.08 | 0.04 | 0.11 |
| 14 | 0.001 | −0.41 | −0.52 | −0.30 | −1.06…0.24 | 0.001 | 0.07 | 0.04 | 0.10 |
| 13 | 0.001 | −0.41 | −0.52 | −0.29 | −1.13…0.32 | 0.001 | 0.11 | 0.08 | 0.15 |
| 12 | 0.001 | −0.20 | −0.31 | −0.09 | −0.88…0.49 | 0.001 | 0.09 | 0.06 | 0.13 |
| 11 | 0.145 | 0.14 | −0.05 | 0.33 | −1.02…1.3 | 0.008 | 0.08 | 0.02 | 0.14 |
| 21 | 0.281 | 0.09 | −0.08 | 0.27 | −0.97…1.16 | 0.001 | 0.07 | 0.05 | 0.09 |
| 22 | 0.001 | −0.19 | −0.30 | −0.08 | −0.84…0.46 | 0.001 | 0.11 | 0.07 | 0.15 |
| 23 | 0.001 | −0.45 | −0.55 | −0.34 | −1.09…0.19 | 0.001 | 0.10 | 0.07 | 0.12 |
| 24 | 0.001 | −0.41 | −0.52 | −0.31 | −1.03…0.2 | 0.001 | 0.08 | 0.05 | 0.11 |
| 25 | 0.001 | −0.23 | −0.33 | −0.13 | −0.85…0.38 | 0.001 | 0.08 | 0.05 | 0.11 |
| 35 | 0.002 | −0.17 | −0.28 | −0.06 | −0.83…0.49 | 0.001 | 0.08 | 0.05 | 0.10 |
| 34 | 0.001 | −0.39 | −0.50 | −0.29 | −1.05…0.26 | 0.001 | 0.11 | 0.07 | 0.16 |
| 33 | 0.102 | −0.09 | −0.19 | 0.02 | −0.71…0.54 | 0.001 | 0.13 | 0.08 | 0.17 |
| 32 | 0.001 | −0.31 | −0.43 | −0.19 | −1.03…0.41 | 0.001 | 0.10 | 0.07 | 0.13 |
| 31 | 0.005 | −0.14 | −0.23 | −0.05 | −0.71…0.43 | 0.001 | 0.08 | 0.05 | 0.11 |
| 41 | 0.019 | −0.13 | −0.25 | −0.02 | −0.82…0.55 | 0.001 | 0.09 | 0.05 | 0.12 |
| 42 | 0.001 | −0.24 | −0.35 | −0.12 | −0.94…0.46 | 0.001 | 0.10 | 0.06 | 0.13 |
| 43 | 0.003 | −0.17 | −0.27 | −0.06 | −0.82…0.49 | 0.001 | 0.12 | 0.08 | 0.16 |
| 44 | 0.001 | −0.45 | −0.53 | −0.37 | −0.93…0.03 | 0.001 | 0.09 | 0.06 | 0.12 |
| 45 | 0.001 | −0.18 | −0.28 | −0.08 | −0.77…0.41 | 0.001 | 0.09 | 0.06 | 0.12 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


