Chapter 40 Radiofrequency tongue base reduction in sleep-disordered breathing
1 INTRODUCTION
1.1 PREOPERATIVE EVALUATION
Sleep-disordered breathing is caused by collapse or obstruction of the upper airway during sleep. This obstruction may occur at any site along the upper airway passages to include the nasal cavity, oropharynx, hypopharynx and larynx. Once the presence of sleep-disordered breathing is documented by a nocturnal polysomnogram and the patient is intolerant of medical therapy, the presurgical evaluation preceeds. The preoperative evaluation includes a comprehensive head and neck physical examination, fiberoptic nasopharyngoscopy and an optional lateral cephalometric radiograph to determine the site or sites of upper airway obstruction. Other diagnostic avenues, such as sleep endoscopy, may also be performed by the surgeon in directing surgical therapy in a site-specific approach. If the base of tongue is determined to be a causative factor in the upper airway collapse, then adding radiofrequency tongue base reduction to the therapeutic regime is contemplated. Numerous surgical procedures have been developed to address each of the sites of obstruction and have offered the surgeon an armamentarium of options, each with its own set of advantages, disadvantages and success rates.
3 OUTLINE OF PROCEDURE: TONGUE BASE RADIOFREQUENCY
The technique can be performed as an outpatient or as an inpatient. Depending on the severity of the patient’s sleep-disordered breathing, post-treatment airway monitoring and/or protection with nasal continuous positive airway pressure (CPAP) or a tracheotomy may be considered.
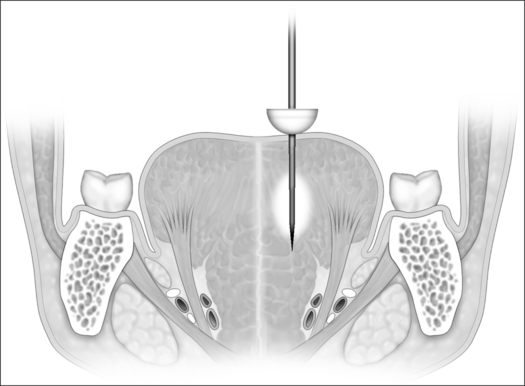
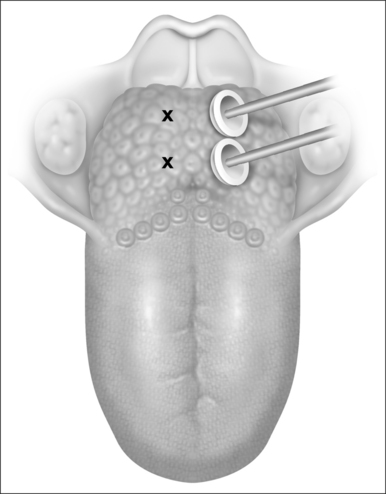
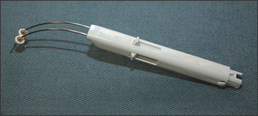
Currently, a dual 22-gauge RF needle electrode with a10 mm active length and a 10 mm protective sheath in a custom-fabricated device allows placement of the electrode under the superficial tongue musculature in the area selected for treatment. Potential sites of treatment include the midline and paramedian dorsal base of tongue areas and the anterior ventral tongue areas (Figs 40.1 and 40.2). Treatment sites should be spaced a minimum of 1.5 cm apart if a single needle probe is used or at least 2.5 cm using the dual needle probe device (Fig. 40.3). Continual pressure on the electrode and visualization that the insulation sheath is not retracting out of the tongue tissue reduce the risk of superficial tissue injury. Using the most current Gyrus radio frequency generator machines and a dual probe at 85°C, 600 joules (J) of rapid energy radiofrequency is delivered to two base of tongue sites with a total of 1200 J delivered. Treatment sessions may be repeated every 4–6 weeks.
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


