Use Extraction Treatment When Necessary
Throughout the history of orthodontics, the pendulum has swung back and forth regarding the extraction of permanent teeth. Clearly, it will never swing back toward the percentage of patients being treated with extractions during the 1950s and 1960s.
In addition to the bonding of brackets, rather than the placement of bands on each tooth, another method to gain space is interproximal enamel reduction. If techniques for transverse expansion are used, 6 to 7 mm of arch length can be gained in selected patients. Therefore, without question many patients who would have been treated with extractions in the past will be treated without extractions today.
The problem now appears to be that some orthodontists have the attitude that every patient, regardless of the severity of crowding, should be treated without extractions, even though the teeth might be placed in unstable positions; these clinicians contend that lifetime retention can resolve this problem. Granted, some patients’ treatment must be compromised when the choice is between esthetics and stability. Happily, this situation does not happen often.
It is true that extraction of any permanent dentition during the course of orthodontic treatment should be avoided whenever possible. However, my experience suggests that approximately 20% of orthodontic patients require extraction of some permanent teeth (other than third molars).
Diagnosis
Premolar extractions
Two types of malocclusion almost always require premolar extractions. In the first type, patients with extreme mandibular arch length discrepancy have more tooth mass than the dental arch can accommodate (Fig 18-1). Regardless of the mechanics used, it would be impossible to gain an adequate amount of space for the dentition to be properly aligned in the arches without extracting teeth.

The mandibular arch is most often the limiting factor in this type of case. In most growing patients, if the mandibular arch can be treated without extraction, so can the maxillary arch. The only routine exception is in a nongrowing Class II patient who does not want surgery. The mandibular arch may be treated as a nonextraction case, while the maxillary premolars are extracted. This treatment eliminates any overjet; the maxillary canines are treated until a Class I relationship is reached, while the molars remain in a Class II relationship (see Principle 18a Case Study). Although it is possible to correct an end-on molar relationship in some patients, it is impractical to attempt significant distalization of molars in most nongrowing patients.
The second type of malocclusion that almost always requires premolar extractions is severe bimaxillary prognathism. In these patients, the mandibular incisors are inclined so far labially that the patient cannot close his or her lips, and the profile is esthetically unappealing (Fig 18-2). In these cases, first premolars are extracted from both arches to create space to retract the maxillary and mandibular anterior teeth into more esthetic positions. Generally, in a patient with bimaxillary protrusion, the incisors can be retracted significantly without causing the face to “dish in.” Class 3 elastics are often used to retract the mandibular anterior teeth.

In any extraction case in which the possibility of a posttreatment concave soft tissue profile appearance exists, extraction of the mandibular second premolars should be considered. This extraction pattern allows for the closure of additional extraction space from the posterior, which prevents the mandibular incisors from moving as far lingually. This treatment regimen may require class 2 elastics during closing mechanics in the mandibular arch to advance the molars, and it is often successful in patients exhibiting slight pretreatment facial convexity and thin attached gingival tissue.
Other extractions
Over the years, I have extracted many different teeth for different reasons. Most often, these extractions have been performed in adult patients.
A single mandibular incisor extraction may be an acceptable treatment option when severe mandibular crowding or flared incisors are present in a patient who has a full Class I molar tendency and small maxillary lateral incisors. Detailed discussion of this topic will be presented in a subsequent volume in this series.
Management of the Extraction Patient
Because of the excessive number of extraction cases treated in the past, the public may be wary when the orthodontist recommends the extraction of teeth. At the initial appointment, a visual examination can determine whether the patient is likely to require extraction. If the problem may require extractions, this information is relayed to the parents and patient immediately. The patient and parents are then prepared if the final preferred treatment plan includes extractions. As with every patient, intraoral photographs are presented at the consultation to illustrate the crowding. It is usually obvious to the family that there is no room for all of the teeth. The precise teeth to be extracted are then indicated.
If the patient exhibits bimaxillary prognathism, the patient’s soft tissue profile is emphasized on the lateral view facial photograph and on the cephalometric tracing. The severe flaring of the incisors is shown. The family is told that after the premolars are removed, the incisors can be uprighted and retracted to achieve a more balanced face and a more stable dental relationship.
The patient and parents must be involved in the extraction treatment decision. If the patient or parent is reluctant to accept extraction treatment, the advantages and disadvantages of each treatment option are explained. For patients with bimaxillary prognathism, there are three advantages to treating the case with extractions:
1. Improved long-term stability of the teeth. The teeth can be straightened without extractions, but the chances of relapse are extremely high.
2. Cosmetic appearance. Without extractions, the results will not be as esthetic at the end of treatment because the teeth will be protruding farther than they should.
3. The health of the teeth and gingival tissue. If the mandibular anterior teeth have to be advanced to avoid extractions, it is possible they could actually be pushed into areas in which less bone and periodontal tissue are available.
After all is said and done, the best way to demonstrate the advantages of extractions for patients with bimaxillary prognathism is to show facial photographs of another patient to demonstrate dramatic profile changes before and after treatment.
After these facts are presented, if the response to extraction treatment is still negative, it is important to write the family’s decision on the treatment card and ask the parents to sign it. Thus, the family has been informed of the potential risks and limitations of nonextraction treatment and has consented to the alternative treatment option. This procedure is a safeguard for the orthodontist.
Typical Extraction Mechanics
Principles
In treating growing children, the orthodontist must always keep in mind that patients are “moving targets.” Whether an extraction or a nonextraction case, the patient is a new person at every appointment. First, he or she is growing; second, orthodontic and orthopedic mechanics are affecting the teeth and the face. Although step-by-step instructions for treatment are provided in this book, alterations in these procedures may be necessary from visit to visit, depending on the patient’s response. The principles are provided; they must be applied to the specific needs of each particular patient:
• Extract all premolars at beginning of treatment.
• Initiate treatment in the maxillary arch.
• Ensure early retraction of canines into a Class I relationship (Fig 18-3).
• Delay treatment in the mandibular arch until the canines are in a Class I relationship.
• Allow the mandibular anterior teeth to drift (“driftodontics”). The exceptions to this rule include adults and patients with Class III occlusions. Often, the mandibular arch is bracketed early in treatment in these cases.

Figs 18-3a to 18-3c Canine retraction on 0.016-inch stainless steel curved archwire with power chains.
Maxillary arch treatment
Initial archwire
As in nonextraction cases, in extraction treatment the initial maxillary archwire is usually a 0.016-inch nickel-titanium wire. Because extraction patients often exhibit more initial crowding in the maxillary arch than do nonextraction patients, this flexible wire is often used for one to two additional appointments. This archwire will correct the crowding, reduce the rotations, and help level the teeth. Because the point of least resistance is toward the extraction site, there is little flaring of the incisors as they align. Most of the tooth movement is into the extraction sites. To make this even more effective, the special low-friction ligation (Fig 18-4) can be placed on those teeth that need the greatest amount of movement.

Second archwire (canine retraction)
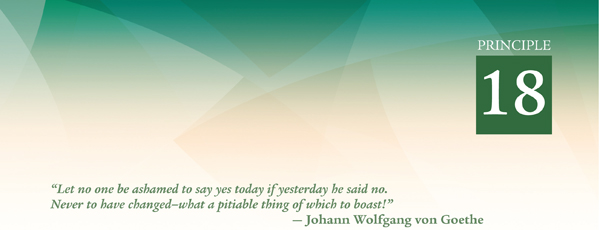
The second archwire is a heat-treated 0.016-inch stainless steel round wire with omega loops. An accentuated curve of Spee may be added to help improve or maintain the overbite (Fig 18-5). The purpose of this wire is to continue arch leveling and eliminate rotations. In addition, this is an excellent wire for retraction of maxillary canines. The distobuccal segments of the archwire entering the first molar buccal tubes are bent parallel to each other (Fig 18-6). These bends, along with the 15 degrees of distal offset built into the first molar tubes, will rotate the molars distobuccally. This will provide cortical anchorage because of the position of the mesiobuccal roots of the first molars in the buccal cortical plate. This anchorage is sufficient to allow the canines to be moved distally while little or no anchorage is lost. Seldom is a transpalatal arch or facebow needed for anchorage.
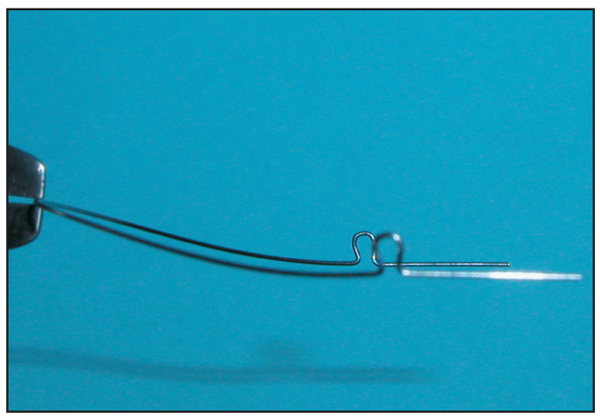
Fig 18-6 Making the distal ends of the archwire parallel to each other will rotate the maxillary first molars easily and accurately.
Maxillary canine retraction has several advantages over en masse retraction:
• Canine retraction can be initiated as early as 2 to 3 months into treatment, rather than at the time of overbite correction.
• There is less anchorage strain and, therefore, no need for a transpalatal arch.
• Later retraction of the four maxillary incisors, as a unit, will control torque much better than en masse movement of all six anterior teeth.
• The amount of space closure is very predictable when closing loops are used, allowing symmetric movement on both sides.
Canine positioning
Maxillary canines are retracted before the incisors. As just mentioned, there are several reasons for this procedure. First, there is greater control over molar anchorage. Only the canines are pitted against the premolars and molars, as opposed to all six anterior teeth. When all six anterior teeth are opposed to four posterior teeth, there is a tendency to lose posterior anchorage. Second, because the canine has the largest root of any tooth in the mouth, it is important to position it as quickly and accurately as possible. The basic goal in this early stage of treatment is to move the canines into a Class I relationship. After that task has been accomplished, it is a matter of bringing all of the remaining teeth together, as the final occlusion is built around the canine position.
Canines can be retracted approximately 1 mm per appointment, every 4 to 6 weeks. Complete canine retraction requires 4 to 6 months on average. Elastomeric chain, attached on each side of the arch from first molar to canine, is used for canine retraction (Fig 18-7). Normally the “short” elastomeric chains are used. Initially, if there is a greater distance from the first molar buccal tube to the canine bracket, four segments of chain are used; otherwise three segments are ideal.

Fig 18-7 (a) Spool of elastomeric chain. (b) Three-unit chain. (c) Elastomeric chain properly attached to canine and first molar.
If there is some initial rotation in the canine, a low-friction ligature tie (a lightly tied steel ligature wire) can be placed on the canine bracket to hold the archwire in the slot. The canine bracket is ligated loosely to reduce any resistance to sliding. The elastomeric chain is then placed over the ligated bracket.
The combination of elastomeric chains and 0.016-inch stainless steel round wires produces a very small amount of friction. This allows canines to be retracted without the need for additional mechanics to control canine torque and rotation. When first applied, an elastomeric chain produces a force of approximately 250 to 300 g. This force dissipates rather quickly over a period of a few days.
Elastomeric chains can cause the canines to rotate and tip distally during the first few days of retraction. Therefore, time-lapse photography of canine retraction would initially show retraction, tipping, and rotation of the canines, as the greater force of the elastomeric chain dominates the archwire force.
Concurrently, as the teeth tip and rotate, the 0.016-inch stainless steel wire in the bracket slot deforms. As the force of the elastomeric chain dissipates, the force of the archwire becomes more dominant. The wire begins to straighten and consequently re-uprights the canine and corrects its rotation. The mesial rotation wing on the Lang brackets will tend to activate the rotation, which returns the canine to its proper position.
Elastomeric chains should not be changed more often than every 4 to 5 weeks. If they are replaced too often, every 2 to 3 weeks, the initial tipping occurs, but the tooth does not have time to upright and rotate itself back into its normal position after the force of the elastomeric chain dissipates. Remember, “let it cook.”
In patients with a Class II skeletal pattern, posterior anchorage during canine retraction is usually supported with a facebow. Omega loops are placed in the 0.016-inch stainless steel round wire. The wire is tied back, and when the patient wears the facebow, an orthopedic effect occurs; the canines are retracted and the molars will not advance. If the patient does not wear the facebow as prescribed, the molars could advance slightly until the molar buccal tubes become flush wi/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


