Introduction
Severe incisor root resorption (SIRR) associated with impacted maxillary canines is rare but has important implications. Early diagnosis and treatment are imperative. In this investigation, we aimed to identify predisposing factors for impacted canine-linked SIRR.
Methods
Clinical and radiographic data of 55 consecutive patients (77 canines) with SIRR of 96 incisors were compared with data from 57 consecutive control subjects (72 canines). The studied variables were age, sex, position of the impacted canine, size of the dental follicle, and incidence of anomalous lateral incisors.
Results
Lateral incisors were more often affected than central incisors, and bilateral SIRR was common. When each variable was examined separately, SIRR was significantly associated with female sex, severely mesiodistally displaced and vertically positioned canines in the middle third of the adjacent incisor root, dental follicles wider than 2 mm, and normal lateral incisors. The multivariate statistical analysis showed that the risk for SIRR was significantly higher in female subjects (4.2 times) with enlarged dental follicles (8.3 times) and normal lateral incisors (5.8 times).
Conclusions
SIRR should be carefully screened in female patients with enlarged dental follicles and normal lateral incisors. A greater degree of canine displacement might also be associated with SIRR.
Highlights
- •
Female patients with enlarged dental follicles and normal lateral incisors should be screened for severe incisor root resorption.
- •
A greater degree of canine displacement might also be associated with severe incisor root resorption.
Early studies with plain film radiography indicated that canine-related incisor root resorption occurs in approximately 12% of patients. Yet the authors were at pains to point out that with plain film radiography, it was impossible to properly assess the buccolingual aspects of the incisor roots. With the advent of more advanced imaging techniques such as computerized tomography scanning, detectable root resorption was diagnosed in 38% of resorbed lateral incisors and 9% of central incisors. Moreover, from the study of Walker et al using cone-beam computed tomography (CBCT), detection capability increased to 67% of cases of which 11% were central incisors and 4% were premolars.
Congenitally missing, small, and peg-shaped maxillary lateral incisors are highly correlated with maxillary canine palatal impaction. Whereas resorption of maxillary incisor roots is a well-recognized phenomenon that can occur in patients with impacted canines, these anomalous lateral incisors with reduced size or abnormal shape have been reported to be less at risk to develop severe root resorption, compared with patients with normally shaped and sized lateral incisors.
Fortunately, severe incisor root resorption (SIRR) associated with impacted maxillary canines is rare, but when is appears, it threatens the long-term survival of the affected teeth. Early diagnosis and treatment are imperative to save the affected tooth. At present, evidence-based information regarding potential predisposing factors for SIRR is lacking.
The aim of this study was to identify predisposing risk factors for SIRR associated with impacted maxillary canines.
Material and methods
The study group included 55 consecutive patients with impacted maxillary canines and SIRR, and the control group included 57 consecutive patients with impacted maxillary canines without SIRR from the Department of Orthodontics of the Hebrew University in Jerusalem, Israel, and the Medical University of Warsaw in Poland and from the private practices of 2 authors (S.C. and A.B.).
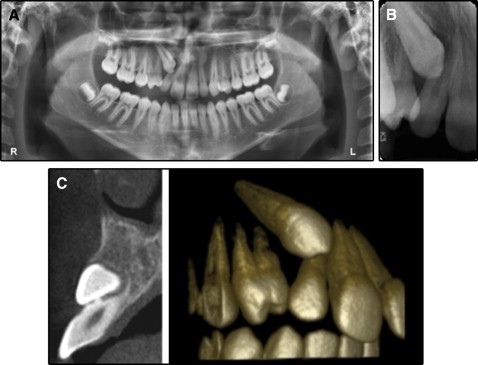
The inclusion criterion for the study group was SIRR of at least 1 maxillary incisor associated with an adjacent impacted canine in untreated healthy patients. Diagnosis of SIRR was made from the available panoramic and periapical radiographs that had been taken earlier with the intention of commencing orthodontic treatment ( Fig 1 , A and B ). For most of the patients (75%) in the study group, CBCT images were also available for examination ( Fig 1 , C ). CBCT was considered superfluous for patients in whom SIRR could be diagnosed on plain films alone. When CBCT was unavailable for a patient, the buccolingual position of the ectopic canine was determined using the routine tube-shift method and confirmed by the treating orthodontist or surgeon during surgical exposure. In the control group, CBCT had been available for all subjects to exclude any signs of root resorption. The radiographs were examined by 2 authors (S.C. and A.B.) using an x-ray viewer with standard light intensity.
The CBCT examinations were performed with an i-CAT scanner (12-bit; Imaging Sciences International, Hatfield, Pa) with the following parameters: 26.9 seconds scan time, 120 kV, 5 mA, field of view size of 13 (height) × 16 (diameter) cm, and 0.2-mm voxel. The resultant slice image data were converted to 3-dimensional images in DICOM format, reconstructed by XoranCat software (version 3.1.62; Xoran Technologies, Inc, Ann Arbor, Mich) and imported to be evaluated in i-CATVision (2008 version 1.8.1.10; Imaging Sciences International). The reconstructed image had a 2-mm slice thickness.
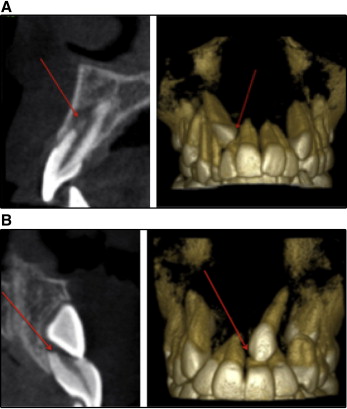
Traditionally, root resorption has been described elsewhere as horizontal shortening of the root. The pattern is different for SIRR associated with impacted maxillary canines, where the resorption is mostly oblique rather than horizontal ( Fig 2 ). Root resorption was measured on the radiographs, and it was considered severe when it affected more than a third of the length of the root, but not specifically its apical part ( Fig 3 ). The exclusion criteria for the sample were root resorption of maxillary incisors less than one third of their expected root length, root resorption secondary to trauma or pulp pathology, or the presence of cysts and other pathologies.

The numbers of involved central vs lateral incisors, and unilateral vs bilateral cases, were recorded.
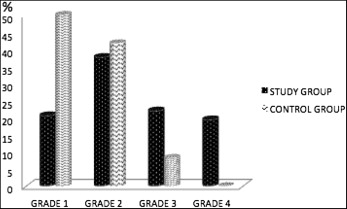
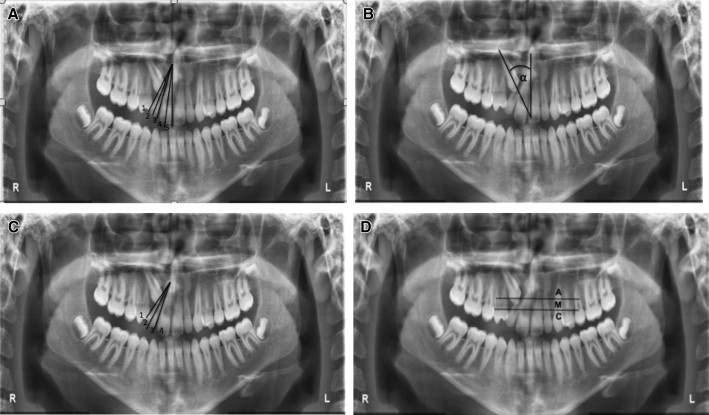
The associations between SIRR and the following variables were evaluated: (1) age; (2) sex; (3) buccolingual location: palatally, buccally, or in the line of the arch; (4) mesiodistal location: sector ( Fig 4 , A ); (5) angulation to the midline ( Fig 4 , B ); (6) overlap of the adjacent incisor ( Fig 4 , C ); (7) vertical crown height relative to the adjacent incisor root: apical, middle, or coronal ( Fig 4 , D ); (8) maximum width of the canine dental follicle graded in 1-mm intervals (0-1 mm, grade 1; 1-2 mm, grade 2; 2-3 mm, grade 3; ≥3 mm, grade 4); and (9) anomalies of the lateral incisors adjacent to the impacted canines (congenitally missing, small, or peg-shaped).
Statistical analysis
The statistical methods for the associations between each variable and SIRR included chi-square tests and logistic regression analyses with SAS software (version 9.4; SAS Institute, Cary, NC) to calculate odds ratios and 95% confidence intervals. A multivariate regression model including 9 categorical variables was performed to identify the significant factors associated with SIRR. Only 1 side was included in the bilateral cases on the advice of the statistician. The inclusion of each side as a separate case was discounted because the 2 sides are not independent variables. The side was chosen at random by the statistician, so that both affected sides had an equal probability to be included in the analysis. All statistical tests were 2 sided at α = 0.05.
Results
In the total study group of 55 patients, there were 96 severely resorbed maxillary incisors—69 lateral and 27 central (ratio 2.5:1)—a difference that was highly statistically significant ( P = 0.001; Table I ). The most frequently resorbed tooth associated with maxillary canine impaction was the maxillary right lateral incisor (41.6%).
| Resorbed maxillary incisor | |||||
|---|---|---|---|---|---|
| Right lateral | Right central | Left central | Left lateral | Total | |
| No. of teeth (%) | 40 (41.6) | 18 (18.8) | 9 (9.4) | 29 (30.2) | 96 (100) |
The study group included 22 patients (20 girls, 2 boys) with bilateral impacted canines, and the control group included 15 bilateral subjects (12 female, 3 male). In the study group among the bilateral impacted canine patients, 3 (13.6%) had unilateral SIRR.
The control group was older than the study group (14.2 ± 4.7 vs 12.0 ± 1.4 years) because of the presence of 3 adults (>20 years old).
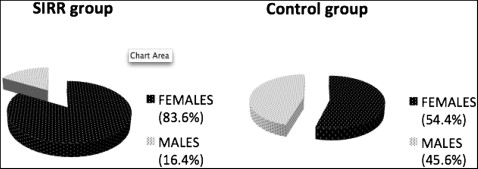
A markedly elevated prevalence of SIRR was associated with maxillary canine impaction in female subjects (83.6% in the study group vs 54.4% in the control group) compared with male subjects (16.4% in the study group vs 45.6% in the control group; P <0.001; Fig 5 ). When studied in isolation, the risk of female patients having SIRR was 4.2 times higher than in males.
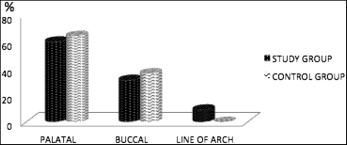
In both groups, the prevalence of palatally impacted canines was higher than that of buccally impacted canines by a ratio just under 2:1 ( Fig 6 ). No statistically significant differences were seen between the study and control groups.
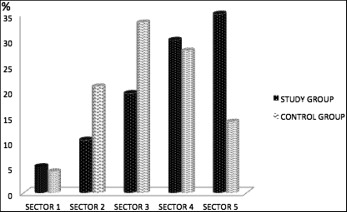
In the study group, most canines (64.9%) were located close to the midline, mainly in sector 5 (35%) and sector 4 (29.9%) ( Fig 7 ). In the control group, only a small percentage of the canines were seen in sector 5 (13.9%), with larger percentages in sectors 3 (33.3%) and 2 (20.8%). The differences between the distributions of canines were almost statistically significant ( P = 0.06). When studied separately, the risk of SIRR in association with canines positioned in sector 5 was 5.5 and 3.5 times higher than for canines positioned in sectors 2 and 3, respectively.
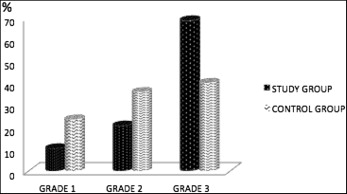
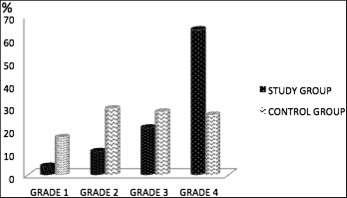
In the study group, 68.8% of the impacted canines were angulated ≥31° (grade 3), 20.8% of the canines were between 16° and 30° (grade 2), and 10.4% of the canines were between 0° and 15° (grade 1) ( Fig 8 ). In contrast, in the control group, only 40.3% of the canines were grade 3, 36.1% were grade 2, and 23.6% were grade 1. The increased prevalence of severely angulated maxillary canines (grade 3) in association with SIRR was statistically significant in comparison with the controls ( P = 0.02). When this factor was studied in isolation, the risk of SIRR associated with a canine in sector 3 was about 3 times more than the risk for SIRR in canines in sectors 1 and 2.
The overlap of the adjacent incisor root was more toward the more extreme end of the grading in the SIRR group, with 64.9% of impacted maxillary canines exhibiting complete overlap of the adjacent root or beyond (grade 4) compared with 26.4% in the control group ( Fig 9 ). Only 14.3% of the canines showed no or less than half root horizontal overlap (grade 1) in the study group, compared with 45.8% in the control group, and the differences were highly statistically significant ( P = 0.001). When studied separately, the risks of SIRR in canines graded 4 were 17.8, 5.8, and 3 times more than in canines graded 1, 2, and 3, respectively.
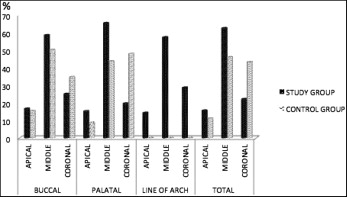
In the vertical plane, more than half (62.3%) of the impacted maxillary canines in the SIRR-affected group were located in the middle third of the adjacent incisor root ( Fig 10 ). Apically positioned crowns of involved maxillary canines comprised 15.6%, and coronally positioned crowns, 22.1% of the total. The differences in the vertical location were highly statistically significant ( P = 0.001). The pattern was different in the control group, with a much higher incidence of coronally positioned crowns (43.1%) and smaller incidences of middle (45.8%) and apical canines (11.1%) compared with the SIRR group ( P = 0.05). When this factor was studied in isolation, the risk of SIRR was 2.7 times higher for a canine in the middle third than for a canine positioned coronally.
The dental follicle was graded 4 (≥3 mm) in 19.5% of the canines in the SIRR group ( Fig 11 ). Grade 4 dental follicles were not observed in any control subject. The differences were statistically significant ( P = 0.03). Grades 3 and 4 dental follicles (≥2 mm) were found in 41.6% of the patients in the study group compared with 8.3% of the subjects in the control group.