This case report presents the clinical features and periodontal findings in a patient with a horizontally impacted maxillary central incisor that had been exposed and aligned after a closed-eruption surgical technique. By combining 3 treatment stages—maxillary expansion, crown exposure surgery, and induced eruption—the horizontally impacted incisor was successfully moved into proper position. The patient finished treatment with a normal and stable occlusion between the maxillary and mandibular arches, and an adequate width of attached gingiva, even in the area surrounding the crown. The 5-year follow-up of stability and periodontal health demonstrated esthetic and functional outcomes after orthodontically induced tooth eruption. Clinical evaluation showed that the treated central incisor had periodontal clinical variables related to visible plaque, bleeding on probing, width of attached gingiva, and crown length that resembled the contralateral incisor.
The problem of an impacted maxillary incisor resulting in space concerns in the anterior region of the early mixed dentition is usually a clinical challenge for orthodontists. Treatment alternatives for an impacted central incisor include (1) induced eruption of the impacted central incisor into its proper position, ie, orthodontically induced tooth eruption ; (2) extraction and space closure by replacing the lateral incisor by the central incisor with subsequent prosthetic restoration ; (3) extraction of the impacted tooth and surgical repositioning of the impacted central incisor ; (4) extraction of the impacted tooth and autotransplantation of a premolar to the region ; and (5) extraction and restoration with an implant or a bridge later when growth has ceased.
Among these, orthodontically induced tooth eruption would be the first choice because of sound evidence of its benefits, since it considers factors such as maintenance of the tooth structure and bone stimulation by movement induction with possible maintenance of alveolar bone width, in addition to the periodontal and esthetic benefits as a whole. Moreover, patients usually want to retain and align the impacted teeth into the proper position despite other treatment alternatives. These treatments might add complexity, requiring a multidisciplinary team, including orthodontist, surgeon, and periodontist.
To accomplish orthodontically induced tooth eruption, the clinician should initially know the etiology of the impaction, aiming at safe planning for removal of the causal factor, space gain in the dental arch, and later induction of eruption.
The authors of previous studies have reported the treatment of impacted incisors with surgical crown exposure and induced eruption, yet they also suggest the need to monitor the stability and periodontal health of the tooth during and after orthodontic treatment. Here we report on an unerupted maxillary central incisor for which traction was used, with special considerations of the surgical technique and the direction of traction.
The overall orthodontic and esthetic outcomes were highly favorable; at the 5-year follow-up of the periodontal status, the central incisor resembled the neighboring homologous tooth.
Diagnosis and etiology
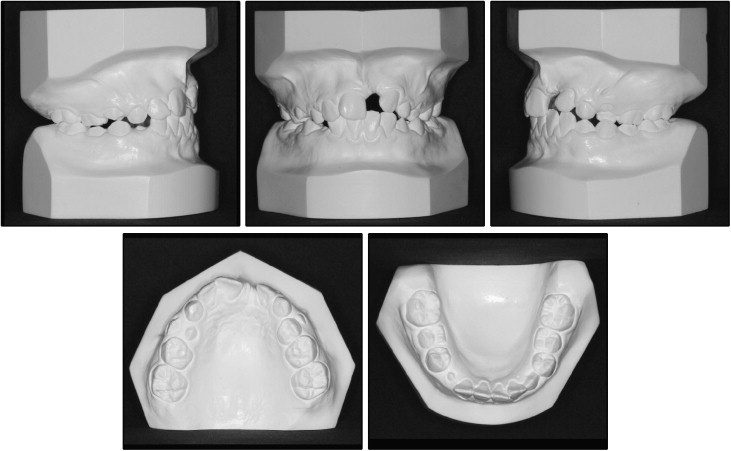
A girl, 8 years 6 months of age, was brought by her parents to the orthodontic clinic of Pontifícia Universidade Católica do Rio Grande do Sul in Porto Alegre, Rio Grande do Sul, Brazil. Their chief complaint was the lack of eruption of the maxillary left central incisor. The facial analysis showed a symmetric face, a balanced facial pattern, and a low smile line with a deficient smile. The intraoral examination showed that the patient was in the early mixed dentition with an Angle Class II molar relationship, and her maxillary left central incisor was missing ( Fig 1 ). A protuberance was observed by palpation of the alveolar mucosa below the nasal spine. The maxillary arch was constricted and V shaped. A left unilateral posterior and anterior crossbite, which extended to the left lateral incisor, was associated with that maxillary constriction. The left lateral and right permanent incisors were tipped palatally and mesially toward the midline, thus occupying part of the central incisor space. There were arch length discrepancies of −6.2 mm in the maxillary arch and −1 mm in the mandibular arch. Overjet and overbite were 3.8 and 3.2 mm, respectively ( Fig 2 ).

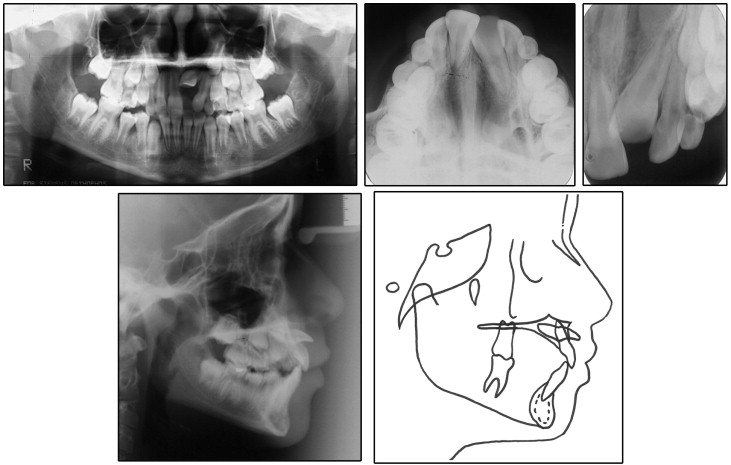
The cephalometric analysis showed a Class I malocclusion: ANB, 4.5°; retroclined maxillary right incisors (1:NA, 3 mm and 15°; 1:NB, 6 mm and 27°; IMPA, 96°); mandibular plane, 34°; and occlusal plane, 19° ( Fig 3 , Table ).
| Measurement | Pretreatment | Posttreatment |
|---|---|---|
| SNA (°) | 80 | 79 |
| SNB (°) | 75 | 78 |
| ANB (°) | 4.5 | 1 |
| 1-NA (mm) | 3 | 7 |
| 1:NA (°) | 15 | 33 |
| 1-NB (mm) | 6 | 6 |
| 1:NB (°) | 27 | 23 |
| 1:1 (°) | 132 | 122 |
| Occl:SN (°) | 19 | 14 |
| GoGn.SN (°) | 34 | 32 |
| S-LS (mm) | 1 | −1 |
| S-LI (mm) | 2 | +1 |
| Y-axis to FH (°) | 59 | 59 |
| NPog.FH (°) | 89 | 89 |
| Angle of convexity (°) | 10 | 1 |
| Wits (mm) | +1 | −2 |
| FMA (°) | 24 | 23 |
| FMIA (°) | 60 | 65 |
| IMPA (°) | 96 | 92 |
| Nasolabial angle (°) | 105 | 108 |
| A-NPerp (mm) | +2 | 0 |
| Co-A (mm) | 81 | 84 |
| Co-Gn | 99 | 113 |
| AIFH (mm) | 56 | 61 |
| Pog-NPerp (mm) | −3 | 0 |
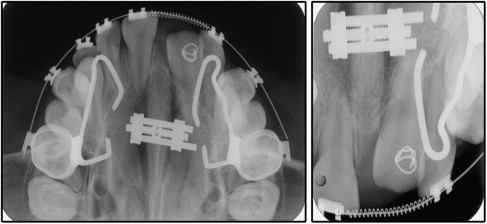
The radiographic findings showed no pathology in the periapical area or root dilaceration of the maxillary left central incisor. The cephalogram demonstrated that the maxillary left central incisor was impacted in a horizontal position in the nasal floor region ( Fig 3 ). It was also possible to determine, with the aid of radiographs, that the crown of the unerupted incisor was positioned in the vestibular sulcus, under the lip frenulum. On complete retraction of the upper lip, the crown tip was clinically palpable in the vestibule.
The parents mentioned that their daughter had experienced trauma at the age of 2 years as the result of a fall that caused premature exfoliation of the maxillary left central deciduous incisor. The child was physically healthy and had no history of medical diseases other than this anterior dental trauma. Impaction and deflection of the maxillary left central incisor are described in the literature as a result of traumatic injury.
Treatment objectives
The following treatment objectives were established: (1) expand the maxillary arch, recovering its ideal form and regaining the space for the maxillary left central incisor; (2) induce eruption for the impacted tooth; (3) orthodontically move the impacted tooth into its original space; (4) create a stable functional occlusion ; (5) establish an esthetic profile; and (6) establish adequate clinical crown length, width of attached gingival levels, and symmetric gingival margins for both maxillary central incisors, while preventing gingival scarring and potential relapse.
Treatment objectives
The following treatment objectives were established: (1) expand the maxillary arch, recovering its ideal form and regaining the space for the maxillary left central incisor; (2) induce eruption for the impacted tooth; (3) orthodontically move the impacted tooth into its original space; (4) create a stable functional occlusion ; (5) establish an esthetic profile; and (6) establish adequate clinical crown length, width of attached gingival levels, and symmetric gingival margins for both maxillary central incisors, while preventing gingival scarring and potential relapse.
Treatment alternatives
- 1.
Orthopedic maxillary expansion and orthodontic space opening, surgical exposure, and orthodontically induced tooth eruption of the horizontally impacted central incisor into its proper position.
- 2.
Extraction of the impacted central incisor and space closure, bringing the lateral incisor into the place of the central incisor and reshaping it by restorative treatment to recreate an ideal central incisor contour.
- 3.
Extraction of the impacted tooth and surgical repositioning of the impacted central incisor.
- 4.
Extraction of the impacted tooth and autotransplantation of a premolar to the region.
- 5.
Extraction of the impacted central incisor, orthodontic space opening, and future restoration with an implant or a prosthetic rehabilitation when growth ceases.
Treatment plan
After discussing the treatment alternatives and the uncertain prognosis, the parents and clinicians chose to try to save the tooth and bring it into its proper position. The treatment was planned in 3 stages. The first stage involved correction of the maxillary deficiency with sufficient maxillary expansion, therefore with correction of the posterior crossbite and space opening to provide adequate space for the maxillary incisor, followed by maxillary stabilization and alignment of the permanent teeth. The second stage consisted of surgical exposure. The third stage comprised traction of the impacted left central incisor from a horizontal to a vertical position and its alignment to obtain a normal occlusal relationship. This stage aimed at finalization and improvement of the occlusion.
Treatment progress
Rapid palatal expansion was performed with a modified Haas appliance, with the maxillary first molars banded because the patient was in the mixed dentition stage. The appliance was initially activated 4 quarter turns (0.8 mm) at cementation, followed by 2 quarter turns per day (0.4 mm) until the posterior crossbite was overcorrected. Afterward, it was maintained for an additional 6 months as a retainer of the expansion and also used as anchorage for the traction.
Next, edgewise brackets were bonded in the maxillary arch, except for the second premolars and the canines, which were erupting, and tooth alignment and leveling began with a 0.014-in nickel-titanium archwire. Leveling of the maxillary anterior teeth was conducted with a 0.016-in stainless steel archwire. A nickel-titanium coil spring was used between the maxillary right central and left lateral incisors to create adequate space for aligning the impacted incisor ( Fig 4 ).