Introduction
The aim of this study was to evaluate the treatment effects of the First Class Appliance (FCA) (Leone, Firenze, Italy) used for the distalization of maxillary first molars in patients with Class II malocclusion and mixed dentition.
Methods
According to the results of the power analysis for sample size calculation, 32 consecutive patients with bilateral Class II molar relationships were initially included in the study. After application of the inclusion and exclusion criteria, 26 patients remained for the final evaluation. They were randomized into 2 groups: treatment group (n = 15) and untreated control group (n = 11). Lateral cephalograms and dental casts were obtained before and immediately after distalization for the treatment group, and initially and approximately 22 weeks later for the control group. Statistical evaluation of the variables included the mixed 2-way analysis of variance at P <0.05. The method error was also estimated.
Results
The mean treatment period to achieve a full Class I molar relationship was 17.2 weeks. Analysis of the data showed significant distalization of the maxillary first molars produced by the FCA (mean: 4.00 mm) when compared with the untreated group (mean: 0.95 mm). The rate of molar movement was 1.00 mm per month, which, however, was associated with distal tipping of the first molars (8.56°) and anchorage loss of the anterior dental unit in terms of overjet increase (0.68 mm), and mesial movement (1.86 mm) and inclination (1.85°) of the first premolars or first deciduous molars. The maxillary first molars also moved buccally (1.37 mm), but no significant distal rotation occurred.
Conclusions
The FCA is an efficient noncompliance appliance to distalize molars in the mixed dentition without distal rotations. However, these movements are associated with distal molar tipping and anchorage loss of the anterior teeth.
A common strategy to treat Class II malocclusions by a nonextraction protocol is to initially distalize the maxillary molars to create a Class I relationship. Various concepts, biomechanics, and appliances have been routinely used, including extraoral traction, removable appliances with springs, and Class II intermaxillary elastics. Since the patients’ compliance is a presupposition for the effectiveness of these modalities, the development and use of techniques and appliances that minimize the need for patient cooperation provides a reliable and more predictable treatment alternative. The category of noncompliance mechanics includes a variety of intramaxillary appliances such as Jones jig, distal jet, pendulum appliance, Keles slider, repelling magnets, compressed coil springs, molar distalizing bows, and orthodontic implants or miniscrew implants.
Noncompliance distalization methods, however, are not problem free. They have some undesirable side effects that diminish their clinical effectiveness, including anchorage loss (posterior: distal molar crown tipping or distal rotation of molar crowns; anterior: mesial movement and proclination of the maxillary anterior teeth). These side effects can vary among the different techniques and appliances, but they are always associated with maxillary molar distalization.
Open-coil springs combined with various noncompliance appliances have been used for a long time to distalize maxillary molars. The First Class Appliance (FCA) (Leone, Firenze, Italy) was recently introduced for unilateral or bilateral noncompliance distalization of the maxillary molars. Until now, only 1 study has examined the effectiveness of this appliance; no evidence-based studies have evaluated its effectiveness in patients in the mixed dentition.
The aim of this randomized controlled clinical trial was to evaluate the dentoalveolar and skeletal treatment effects of the FCA when used for distalization of the maxillary first molars in patients with Class II malocclusion in the mixed dentition.
Material and methods
The sample size of this investigation was calculated with a power analysis that evaluated the primary hypothesis concerning the interaction effect (time × group) with η 2 = 0.1, correlation coefficient = 0.5, and probability of type I error, α = 0.05. The power analysis showed that 26 patients were needed to achieve 89% power to detect clinically meaningful differences of the tooth movements between the 2 groups. To compensate for possible dropouts during the trial, we decided to enroll more patients.
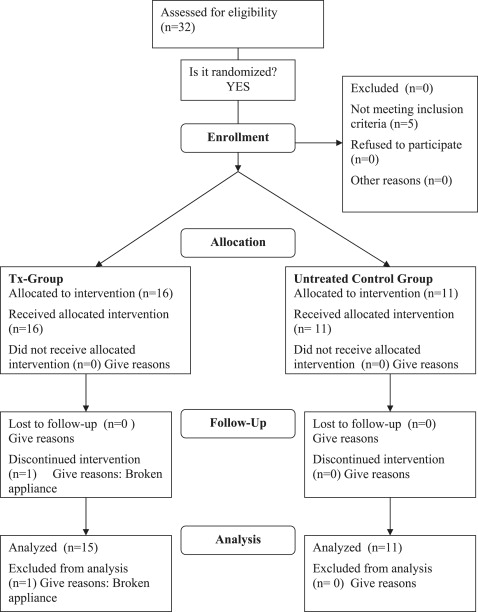
Therefore, 32 consecutive patients with Class II malocclusion were included in the study. They were randomized into 2 groups. The treatment group (n = 16) received the FCA for the first phase of the overall treatment, and the untreated control group (n = 16) received no orthodontic treatment during the examination period. All patients were in the mixed dentition and were treated at the Department of Orthodontics, School of Dentistry, Aristotle University of Thessaloniki in Greece.
To be included in the study, all patients had bilateral Class II molar relationships (quarter to 1 molar cusp). Exclusion criteria included past orthodontic treatment, crossbites, severe carious lesions, poor oral hygiene, mobility of the maxillary deciduous second molars, flat palate, ectopic maxillary canines, anterior open bites, vertical growth pattern, and tongue habits.
Five patients from the control group not meeting the inclusion criteria were excluded from the study, and 1 patient in the treatment group was also excluded because the appliance broke. Therefore, from the treatment group, 15 patients remained for final evaluation, and, from the untreated control group, there were 11 subjects ( Fig 1 ).
In the treatment group with the FCA, 9 patients had a half-cusp molar relationship, 3 had a three quarters-cusp molar relationship, and 3 had a full-cusp molar relationship. In the untreated control group, 2 individuals had a quarter-cusp molar relationship, 5 had a half-cusp molar relationship, 3 had a three quarters-cusp molar relationship, and 1 had a full-cusp molar relationship. The patients in the FCA group received no treatment for the mandible during the examination period.
Informed consent was signed by all parents or guardians of the patients after they received detailed information about the planned clinical trial and their children’s future orthodontic treatment. The trial was approved by the ethical committee of the School of Dentistry of the Aristotle University of Thessaloniki and was conducted according to its guidelines.
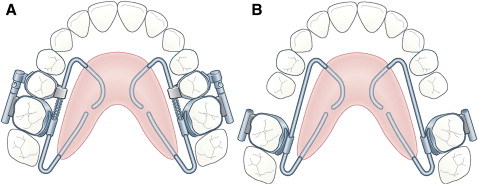
The FCA consists of 4 bands (2 on the maxillary first molars and 2 on either the second deciduous molars or the maxillary second premolars), 2 buccally positioned activation screws (10 mm long) that are soldered to the first molar bands and seated into closed rings welded to the second deciduous molar or the second premolar bands, two 0.010 × 0.045-in palatally positioned open nickel-titanium coil springs (10 mm long), buccal and palatal tubes, and a large modified Nance butterfly-shaped button ( Fig 2 , A ).
Two 0.045-in wires embedded in the acrylic connect the Nance button with the bands. These wires are soldered to the palatal surfaces of the second deciduous molar or the premolar bands and placed into 0.045-in tubes welded to the palatal surfaces of the first molar bands. The Nance button is large to enhance anchorage control during the active phase of treatment and the retention phase that follows. The open nickel-titanium coil springs are fully compressed between the solder joint on the second deciduous molar or the premolar bands and the tube on the first molar bands.
The patients’ guardians activated the appliance by turning the buccally positioned screws a quarter turn in a counterclockwise direction once a day (widening of 0.1 mm). Distal molar movement takes place in a “double-track” system that might prevent rotation of the molars. The palatally positioned nickel-titanium coil springs deliver a force of 200 g. However, the amount of force is not of significant importance because the activation of the coil springs just follows and is limited by the activation of the buccally positioned screws; thus, the springs do not play an active role during molar distalization. The continuous forces exerted by the springs aim to counterbalance the action of the screws, preventing molar rotation during distalization.
After banding the FCA ( Fig 3 , A and B ) , activation of the left and right screws of a quarter turn per day (0.1 mm lengthening) was instructed. After distalization ( Fig 3 , C ), the FCA could be modified to a Nance button for retention ( Fig 2 , B ). However, in this study and for oral-hygiene reasons, it was decided to remove the appliance after distalization and replace it with a new Nance button, acting as a retention device until eruption of all permanent teeth.

Lateral cephalometric radiographs and dental casts were obtained for the treatment group before and immediately after distalization (mean age at treatment start, 9.2 years) and the control group initially and approximately 22 weeks later (mean age at start, 9.7 years).
All lateral cephalometric radiographs were taken by one author (A.B.M.) with the same conditions and the same device. The radiographic magnification factor (10%) was constant for all radiographs. They were traced, digitized, and analyzed by the same author using the scanner Scanmaker 9800 XL (Microtek, Cerritos, Calif) and the cephalometric software Viewbox 3 (dHal Software, Kifissia, Greece) after appropriate adjustment.
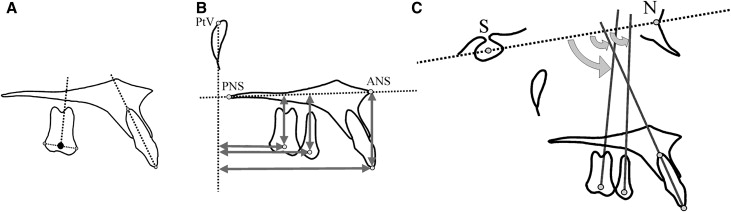
In total, 67 cephalometric points were used. Evaluation of dentoalveolar and skeletal changes was made with 17 variables ( Table I ). Six angular measurements were used to assess skeletal changes ( Table I ). Dentoalveolar measurements included 3 angular and 8 linear variables ( Table I ). A point at the center of the posterior teeth (centroid), was used to determine their actual position in the sagittal and the vertical planes. This point represents the midpoint between the greatest mesial and distal convexity of the crowns as seen on the cephalometric radiograph ( Fig 4 , A ) . To assess the dental changes in the horizontal and sagittal planes, measurements were made from the centroid points of the premolars and molars and from the incisor tip to the pterygoid vertical (PTV) and palatal (ANS-PNS) reference planes, respectively ( Fig 4 , B ). The long axes of the premolars and molars were constructed by drawing a perpendicular from the centroid to a line connecting the most convex points of the crowns of those teeth. Angular changes were estimated with reference to the inclination of the long axes to the sella-nasion (SN) plane ( Fig 4 , C ). In case of double projection of the molars or premolars, a medial contour was traced and used for the corresponding measurements.
| Variable | Treatment group (n = 15) | Control group (n = 11) | Significance | Error of the method | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | P | s(i) | |
| Cephalometric variables | ||||||
| Skeletal angular measurements (sagittal) | ||||||
| SNA (°) | 82.16 | 3.33 | 80.98 | 3.75 | 0.416 | 0.29 |
| SNB (°) | 76.32 | 2.83 | 74.81 | 4.16 | 0.290 | 0.03 |
| ANB (°) | 5.85 | 2.11 | 6.18 | 2.40 | 0.717 | 0.10 |
| Skeletal angular measurements (vertical) | ||||||
| SN-palatal plane (°) | 8.31 | 3.25 | 8.15 | 3.56 | 0.903 | 0.01 |
| SN-mandibular plane (°) | 33.39 | 4.92 | 35.45 | 7.23 | 0.407 | 0.08 |
| SN-occlusal plane (°) | 21.36 | 4.99 | 22.00 | 4.74 | 0.747 | 0.17 |
| Dentoalveolar angular measurements | ||||||
| SN- 6 (°) | 115.93 | 6.91 | 118.27 | 6.78 | 0.405 | 0.08 |
| SN- 5 or SN- E (°) | 115.71 | 5.64 | 113.82 | 6.97 | 0.459 | 0.15 |
| SN- 1 (°) | 74.64 | 11.19 | 77.73 | 5.48 | 0.412 | 0.07 |
| Dentoalveolar linear measurements (sagittal) | ||||||
| PTV- 6 centroid (mm) | 20.04 | 4.37 | 19.05 | 2.40 | 0.507 | 0.04 |
| PTV- 5 or PTV- E centroid (mm) | 30.32 | 5.01 | 29.41 | 2.08 | 0.578 | 0.15 |
| PTV- 1 (mm) | 58.36 | 8.22 | 57.95 | 4.03 | 0.883 | 0.04 |
| Overjet (mm) | 6.75 | 2.72 | 6.32 | 2.80 | 0.710 | 0.01 |
| Dentoalveolar linear measurements (vertical) | ||||||
| Palatal plane- 6 centroid (mm) | 15.00 | 1.93 | 16.18 | 3.72 | 0.314 | 0.03 |
| Palatal plane- 5 or palatal plane- E centroid (mm) | 18.61 | 2.13 | 20.27 | 3.29 | 0.139 | 0.01 |
| Palatal plane- 1 (mm) | 28.93 | 5.69 | 30.00 | 3.91 | 0.599 | 0.01 |
| Overbite (mm) | 5.64 | 1.23 | 4.64 | 3.36 | 0.114 | 0.02 |
| Dental cast variables | ||||||
| 6 -RP (mm) | 23.35 | 1.62 | 23.16 | 1.74 | 0.776 | 0.02 |
| 5 -RP or E-RP (mm) | 13.35 | 1.58 | 13.66 | 1.82 | 0.648 | 0.10 |
| 6 -ML (mm) | 21.98 | 1.14 | 22.41 | 0.92 | 0.317 | 0.05 |
| 6 -ML rotation (°) | 33.77 | 5.04 | 28.82 | 3.87 | 0.012 ∗ | 0.10 |
| 1 -RP (mm) | 11.07 | 2.20 | 11.14 | 1.89 | 0.933 | 0.05 |
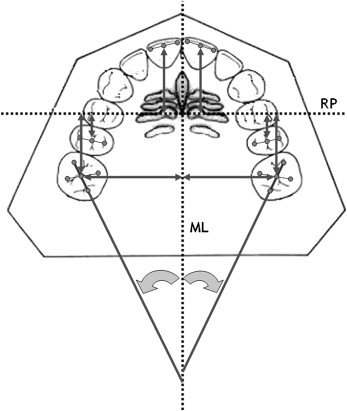
Regarding the measurements on the dental casts, the procedures described by Erverdi et al and Champagne were followed. The palatal rugae and medial palatal suture were traced by using a 0.5-mm point drawing pencil. The most prominent rugae close to the midline and the cusp tips of the molars, incisors, and premolars were marked.
Reference lines (midpalatal line, ML) and planes (rugae plane, RP) were constructed to evaluate molar, premolar, and incisor changes in the sagittal plane ( 6 -RP, 5 -RP, or E -RP and 1 -RP, respectively), molar movement in the transverse plane ( 6 -ML), and molar rotation ( 6 -ML rotation) ( Fig 5 ). Measurements were made separately for the left and right teeth; their average was used for the statistical analysis.
To estimate the error of the method, 26 randomly chosen cephalometric radiographs and dental casts were traced, digitized, and analyzed again by the same examiner within 40 to 60 days after the first assessment. The magnitude of the method error was estimated according to Dahlberg’s formula.
Statistical analysis
The differences between the 2 groups before treatment were compared with the Fisher’s Exact-test for the qualitative variables (male-to-female ratio) and the Student’s t test for the quantitative variables (age).
The normality assumption of the data was evaluated with the Shapiro-Wilk’s test; homogeneity of the variables was assessed by using the Levene’s test.
According to this evaluation, the differences of the variables between before and after treatment for the treatment group and between the initial and final measurements of the control group were compared with the mixed 2-way analysis of variance (ANOVA) with repeated measurements. The same test was also used to compare the treatment or growth changes between the 2 groups.
Statistical analysis was performed using the SPSS software for Windows (version 12.0, SPSS, Chicago, Ill). The level of significance for all tests was set at P <0.05.
Results
The maxillary first molars were distalized into a Class I relationship in all patients. The mean treatment period to achieve a full Class I molar relationship was 17.2 weeks (4.01 months).
The estimated error of the method is listed in Table I . Demographic data of the 2 groups of patients are shown in Table II . No differences were found in the male-to-female ratio ( P = 1.000) and the mean age before treatment ( P = 0.205) between the groups.
Pretreatment and posttreatment means and standard deviations of the variables under investigation for the 2 groups, their differences, and their statistical significances are listed in Tables I and III through V .
| Variable | T1 | T2 | Difference of means | Significance | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | (T2-T1) | P | |
| Cephalometric variables | ||||||
| Skeletal angular measurements (sagittal) | ||||||
| SNA (°) | 82.16 | 3.33 | 82.29 | 3.29 | 0.13 | 0.799 |
| SNB (°) | 76.32 | 2.83 | 76.46 | 2.50 | 0.14 | 0.756 |
| ANB (°) | 5.85 | 2.11 | 5.84 | 1.76 | –0.01 | 0.957 |
| Skeletal angular measurements (vertical) | ||||||
| SN-palatal plane (°) | 8.31 | 3.25 | 7.51 | 2.64 | –0.80 | 0.195 |
| SN-mandibular plane (°) | 33.39 | 4.92 | 35.45 | 4.70 | 1.05 | 0.118 |
| SN-occlusal plane (°) | 21.36 | 4.99 | 21.36 | 5.42 | 0.00 | 1.000 |
| Dentoalveolar angular measurements | ||||||
| SN- 6 (°) | 115.93 | 6.91 | 124.49 | 6.02 | 8.56 | 0.000 † |
| SN- 5 or SN- E (°) | 115.71 | 5.64 | 113.86 | 6.59 | –1.85 | 0.297 |
| SN- 1 (°) | 74.64 | 11.19 | 72.64 | 11.28 | –2.00 | 0.059 |
| Dentoalveolar linear measurements (sagittal) | ||||||
| PTV- 6 centroid (mm) | 20.04 | 4.37 | 16.04 | 4.00 | –4.00 | 0.000 † |
| PTV- 5 or PTV- E centroid (mm) | 30.32 | 5.01 | 32.18 | 4.77 | 1.86 | 0.001 † |
| PTV- 1 (mm) | 58.36 | 8.22 | 59.96 | 8.05 | 1.60 | 0.065 |
| Overjet (mm) | 6.75 | 2.72 | 7.43 | 3.06 | 0.68 | 0.039 ∗ |
| Dentoalveolar linear measurements (vertical) | ||||||
| Palatal plane- 6 centroid (mm) | 15.00 | 1.93 | 13.89 | 2.99 | –1.11 | 0.081 |
| Palatal plane- 5 or palatal plane- E centroid (mm) | 18.61 | 2.13 | 18.68 | 2.41 | 0.07 | 0.867 |
| Palatal plane- 1 (mm) | 28.93 | 5.69 | 29.11 | 6.09 | 0.18 | 0.567 |
| Overbite (mm) | 5.64 | 1.23 | 5.07 | 1.36 | –0.57 | 0.017 ∗ |
| Dental cast variables | ||||||
| 6 -RP (mm) | 23.35 | 1.62 | 27.08 | 2.67 | 3.73 | 0.000 † |
| 5 -RP or E -RP (mm) | 13.35 | 1.58 | 11.87 | 2.19 | –1.48 | 0.000 † |
| 6 -ML (mm) | 21.98 | 1.14 | 23.35 | 1.17 | 1.37 | 0.000 † |
| 6 -ML rotation (°) | 33.77 | 5.04 | 34.67 | 5.00 | 0.90 | 0.051 |
| 1 -RP (mm) | 11.07 | 2.20 | 11.13 | 2.22 | 0.06 | 0.675 |
| Variable | T1 | T2 | Difference of means | Significance | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | (T2-T1) | P | |
| Cephalometric variables | ||||||
| Skeletal angular measurements (sagittal) | ||||||
| SNA (°) | 80.98 | 3.75 | 80.70 | 3.24 | –0.28 | 0.621 |
| SNB (°) | 74.81 | 4.16 | 75.64 | 4.07 | 0.83 | 0.102 |
| ANB (°) | 6.18 | 2.40 | 5.38 | 2.64 | –0.80 | 0.012 |
| Skeletal angular measurements (vertical) | ||||||
| SN-palatal plane (°) | 8.15 | 3.56 | 7.45 | 3.41 | –0.70 | 0.311 |
| SN-mandibular plane (°) | 35.45 | 7.23 | 35.49 | 7.47 | 0.04 | 0.951 |
| SN-occlusal plane (°) | 22.00 | 4.74 | 21.64 | 3.89 | –0.36 | 0.631 |
| Dentoalveolar angular measurements | ||||||
| SN- 6 (°) | 118.27 | 6.78 | 116.82 | 5.04 | –1.45 | 0.391 |
| SN- 5 or SN- E (°) | 113.82 | 6.97 | 114.55 | 5.15 | 0.73 | 0.715 |
| SN- 1 (°) | 77.73 | 5.48 | 78.18 | 6.08 | 0.45 | 0.693 |
| Dentoalveolar linear measurements (sagittal) | ||||||
| PTV- 6 centroid (mm) | 19.05 | 2.40 | 19.09 | 2.55 | 0.04 | 0.936 |
| PTV- 5 or PTV- E centroid (mm) | 29.41 | 2.08 | 29.77 | 2.46 | 0.36 | 0.497 |
| PTV- 1 (mm) | 57.95 | 4.03 | 58.23 | 4.61 | 0.28 | 0.774 |
| Overjet (mm) | 6.32 | 2.99 | 5.82 | 2.80 | –0.50 | 0.165 |
| Dentoalveolar linear measurements (vertical) | ||||||
| Palatal plane- 6 centroid (mm) | 16.18 | 3.72 | 16.64 | 2.72 | 0.46 | 0.514 |
| Palatal plane- 5 or palatal plane- E centroid (mm) | 20.27 | 3.29 | 20.23 | 2.98 | –0.04 | 0.925 |
| Palatal plane- 1 (mm) | 30.00 | 3.91 | 30.23 | 3.88 | 0.23 | 0.519 |
| Overbite (mm) | 4.64 | 3.36 | 4.64 | 2.36 | 0.00 | 1.000 |
| Dental cast variables | ||||||
| 6 -RP (mm) | 23.16 | 1.74 | 23.55 | 1.40 | 0.39 | 0.425 |
| 5 -RP or E -RP (mm) | 13.66 | 1.82 | 13.61 | 1.73 | –0.05 | 0.894 |
| 6 -ML (mm) | 22.41 | 0.92 | 22.43 | 0.96 | 0.02 | 0.823 |
| 6 -ML rotation (°) | 28.82 | 3.87 | 28.86 | 3.60 | 0.04 | 0.930 |
| 1 -RP (mm) | 11.14 | 1.89 | 10.86 | 2.16 | –0.28 | 0.150 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


