Armamentarium
|
History of the Procedure
For history and evolution of the maxillectomy procedure, please refer to the discussion of partial/infrastructure maxillectomy in Chapter 84 .
History of the Procedure
For history and evolution of the maxillectomy procedure, please refer to the discussion of partial/infrastructure maxillectomy in Chapter 84 .
Indications for the Use of the Procedure
Complete unilateral maxillectomy or one of its variants is commonly performed for surgical resection of benign or malignant tumors of the maxilla, whether they originate from bone, minor salivary glands, sinus tissue, or dental tissues. The comprehensive treatment of malignant diseases of the maxilla commonly entails a combined approach utilizing adjuvant radiotherapy or chemotherapy, especially when dealing with advanced stage disease. Surgical resection is the treatment of choice for the majority of these tumors, except for those that are highly responsive to radiotherapy or chemotherapy, such as lymphoreticular malignancies.
Surgical resection of the maxilla and its contiguous structures can be divided into three main types: partial maxillary resection with the preservation of the roof and superior portions of the antrum, total maxillary resection with preservation of the globe, and total maxillary resection with orbital exenteration. The precise limit of surgical resection is determined by the extent of the tumor.
Determination of the extent of resection is especially challenging in the preoperative evaluation of maxillary tumors, as the bulk of the tumor is rarely visualized during physical examination. Preoperative evaluation should include a standard head and neck examination, focused on the oral cavity, nasal cavity, and orbital regions. Flexible nasopharyngoscopy can provide more thorough visualization of the nasal cavity, nasopharynx, and oropharynx and has become a standard adjunct to clinical head and neck examination. Imaging studies such as computed tomography (CT) scans and magnetic resonance imaging (MRI) when correlated with clinical examination will help stage the tumors accurately. Ohngren’s line is actually an imaginary plane drawn from the medial canthus to the angle of the mandible ( Figure 101-1 ) .
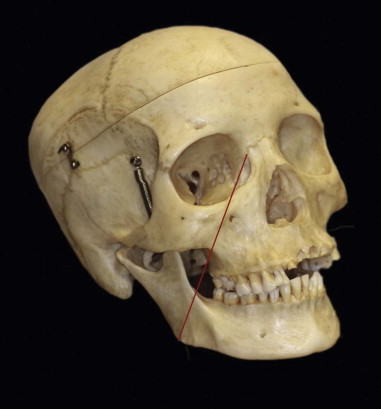
This plane roughly divides the maxillary sinus into an anteroinferior aspect and a posterosuperior aspect. Not surprisingly, tumors that are located within or have extended into the posterosuperior aspect of the maxillary sinus tend to be associated with a poor prognosis, as they are more likely to exhibit involvement of the orbit and infratemporal fossa. Obvious signs of invasion of orbital contents include proptosis and impairment of extraocular muscle function that will necessitate orbital exenteration for complete resection of the lesion. Ophthalmologic consultation is frequently helpful when trying to ascertain if orbital contents have been invaded, and it is especially valuable to assess the status of the opposite eye.
Total ipsilateral maxillary resection is not always required. Tumors originating from the inferior aspect of the maxilla or maxillary sinus (below Ohngren’s line) can commonly be treated with a partial maxillectomy involving the inferior portion of the maxilla, thereby preserving the zygomatic complex, the orbital floor, and the inferior orbital rim ( Chapter 84 ). Likewise, tumors involving only the medial maxillary wall or lateral nasal wall, such as an inverted papilloma, can be treated with a medial maxillectomy. Bilateral, total maxillectomy is occasionally required and entails much greater complexity in reconstruction. A variety of vascularized bone flaps can be utilized, as can support of an obturator prosthesis on four zygomatic implants. On occasion, the tumor will have extended beyond the confines of the maxillary antrum into adjacent structures such as the ethmoid sinus, sphenoid sinus, pterygomaxillary and infratemporal fossae, and the orbit. Extended maxillectomy or craniofacial resection may be required, if the tumor is resectable.
Benign and malignant tumors of the maxilla and maxillary sinuses are histologically diverse, as they arise from varied structures. They can arise from within the Schneiderian membrane, from the bone surrounding the maxillary sinus, from odontogenic tissues within the alveolar process, or can extend into the maxilla or maxillary sinus through contiguous spread from surrounding structures such as the oral cavity, orbit, nasopharynx, skull base, or overlying skin. Evaluation of patients with these tumors requires three-dimensional imaging, and both MRI and CT scans are helpful in discriminating the extent of tumor mass from backed-up secretions within the maxillary sinus lumen or within adjacent paranasal sinuses. Ideally, a multidisciplinary team is required to provide comprehensive evaluation, treatment, and adjunctive therapy, but unfortunately it is often the case that not all specialists are available for every patient.
Limitations and Contraindications
The decision to perform surgery is based on the type and extent of the tumor and the patient’s general health, comorbidities, and wishes. Absolute contraindications for performing a maxillectomy include the patient’s refusal to provide consent for surgery, diseases such as lymphoreticular tumors that are best treated by nonsurgical means, or a debilitated patient who is unable to tolerate surgery due to poor overall health. Relative contraindications center on situations where maxillectomy with curative intent may not be feasible and a palliative course of treatment may be preferable. Such situations may involve patients with untreatable distant metastases. A palliative treatment plan may be more appropriate for patients with large tumors that require bilateral orbital exenteration and for tumors with extensive intracranial invasion.
Technique: Total Ipsilateral Maxillectomy with Orbital Preservation via Weber-Ferguson Approach
The Weber-Ferguson surgical approach is indicated for access to maxillary tumors that either extend superiorly toward the orbital floor or involve the orbit or for tumors that extend posteriorly toward the posterior wall of the maxillary antrum. This approach provides a wide access to all areas of the maxilla and orbital floor.
Step 1:
Patient Preparation
Oral-endotracheal intubation with a reinforced tube is a standard airway for maxillectomy, although contralateral nasal endotracheal intubation can be used for unilateral maxillectomy. A tracheotomy is always appropriate and is recommended for extended maxillectomy and for maxillectomy along with a craniofacial resection. Hypotensive anesthesia to minimize blood loss is advisable. Preoperative packing of the nasal cavity with decongestant-soaked materials and regional injection of epinephrine-containing local anesthesia in a manner similar to that for a septorhinoplasty can reduce blood loss. The eye is protected with a temporary 5-0 silk tarsorrhaphy suture prior to incision if orbital preservation is planned.
Step 2:
Skin Incisions
An incision line is drawn along the crest of the ipsilateral philtral column of the lip from the nostril sill inferiorly to the white roll. The incision then turns medially 90 degrees and is extended within the white roll to the midline of Cupid’s bow. Here, the incision line turns inferiorly 90 degrees to extend through the vermillion of the lip, thereby creating a step-off, which will resist scar contracture and subsequent notching of the lip. Creation of a Z-plasty on the mucosal inner surface of the lip at the time of closure also helps avoid notching. From the superior extent of the philtral column incision at the nostril sill, the incision line turns 90 degrees laterally to extend around the base of the nose, and superiorly along the nasofacial groove (at the border of the aesthetic units) terminating just below the medial canthus. This incision will be adequate for most maxillectomies. If further lateral release is needed, the subciliary extension can be created. The incision line is drawn extending laterally within a skin crease approximately 3 to 4 mm below the ciliary line to just below the lateral canthus. This incision line can be modified to extend further laterally or superiorly as required for tumor removal.
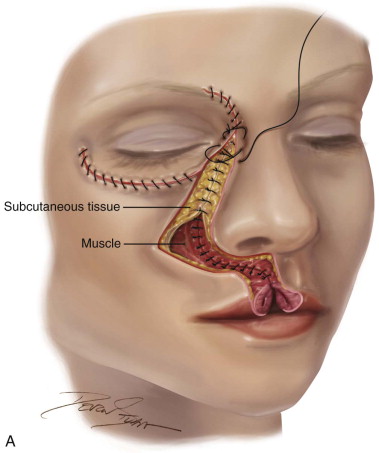
A #15 blade is then used to make the lateral rhinotomy portion of the incision. Skin and subcutaneous tissue are incised along the nasofacial groove and the incision is brought inferiorly, transecting the full thickness of the upper lip through the vermilion. The superior labial artery is ligated or coagulated. The subciliary incision of the Weber-Ferguson approach is then begun laterally at the lateral canthus and is brought medially in the subciliary level, approximately 3 to 4 mm below the lower eyelid and extended slightly inferior to the medial canthus toward the superior end of the lateral rhinotomy incision. The underlying orbicularis oculi muscle is then incised in a tangential direction and directed inferiorly down to bone in a preseptal plane, utilizing electrocautery. This method of incision through the orbicularis oculi muscle will maintain the integrity of the orbital septum ( Figure 101-2, A ).

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


