Chapter 51 Hyo-mandibular suspension and hyoid expansion for obstructive sleep apnea
1 INTRODUCTION
Upper airway obstruction results from excess and/or collapse of soft tissue in the soft palate, tonsillar pillars, tongue, tongue base, and hypopharyngeal walls. Specific anatomic risk factors predisposing to obstructive sleep apnea/hypopnea syndrome (OSAHS) include long soft palate, shallow palatal arches, large tongue base, narrowmandibular arches, and mandibular hypoplasia.1 Othergeneral anatomic factors often associated with OSAHS include obesity, large Body Mass Index (BMI), shortened thick neck, anterior larynx location, enlarged tonsils and/or adenoids, lingual tonsils, thickened pharyngeal walls, elongated uvula, redundant soft palate, large tonguevolume, deviated nasal septum, turbinate hypertrophy, and redundant or folded epiglottis.2 Cephalometric studies employing computed tomography (CT) have correlated increased OSAHS severity with increased BMI, larger tongue and soft palate volumes, and decreasedairway space.3 Diagnostically, Fujita employed endoscopy with the Mueller maneuver (reverse Valsalva) to identify sites of obstruction in the nasopharynx, oropharynx and hypopharynx.4 Three general profile types were identified based on the predominant areas of obstruction:Type I – retropalatal/velopharyngeal; Type II – retropalatal/velopharyngeal and hypopharyngeal; and Type III –hypopharyngeal. Catheter pressure transducers employed in OSA sleep studies have shown that upper airway collapse occurred at the velopharyngeal/retropalatal level and the hypopharyngeal/postlingual level in comparable frequencies.5
2 OPERATIVE PROCEDURES
2.1 HYO-MANDIBULAR SUSPENSION
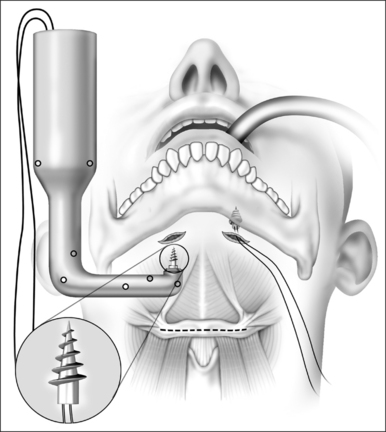
The anterior neck is prepped and draped. The anterior mandible, hyoid and the thyroid cartilages are then outlined with a skin marker with the neck slightly extended. Lidocaine with epinephrine 1:100,000 is injected into the planned incision sites. Two 0.5 cm incisions are made under the chin off the midline and using blunt dissection, the soft tissues overlying the mandible are cleaned. After insertion of the first screw using the Repose device (Influent, Concord, NH), the screw inserter is loaded with a new spare screw and the inserter is positioned perpendicular to the mandible, firm pressure applied and the screw is inserted into the inferior edge of the mandible. A loop of #1 polypropylene suture is already preloaded to the screw by the manufacturer (Fig. 51.1).
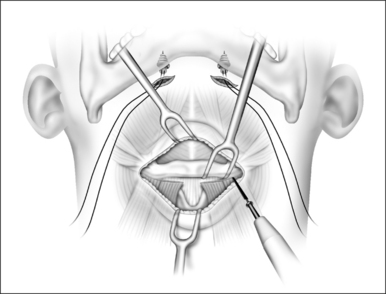
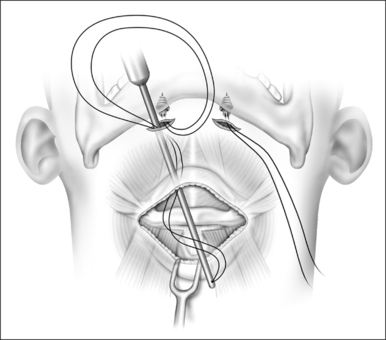
A second horizontal incision is made over the body of the hyoid measuring 5–6 cm. Subcutaneous fatty adipose tissue can be dissected and removed. Electrocautery is used to separate the infrahyoid muscles from the body of the hyoid bone. A single bone hook is placed to retract and stabilize the hyoid during the dissection. The sternohyoid and thyrohyoid muscles are detached from the body of the hyoid between the lesser cornuae (Fig. 51.2). Careful dissection around the body of the hyoid eliminates risk of injury to the neurovascular structures. Careful dissection and good hemostasis are mandatory to avoid injury to the pre-epiglottic fat pad. The suture passer is then loaded with the polypropylene suture and tunneled at the subplatysma layer from the mandibular incisions into the lower (hyoid) incision (Fig. 51.3). The suture passer is then removed. One free end of the polypropylene suture is then loaded into a Mayo needle and is passed through the suprahyoid muscles, catching a full thickness bite of the tissue.
2.2 HYOID DISTRACTION AND EXPANSION
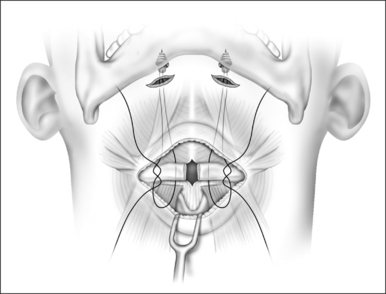
When the hypopharyngeal airway needs to be enlarged in a lateral direction, as determined by preoperative fiberoptic endoscopy, the hyoid bone is then divided in the midline (hyoid distraction) (Fig. 51.4). Following the division of the hyoid bone the polypropylene suture is passed around both sides of the divided edges in a figure of eight configuration (Fig. 51.5). The distracted hyoid segments are then prepared for suspension toward the mandible. In order to maintain stability of the two hyoid segments an absorbable or non-absorbable rigid or semirigid implant can be placed to keep the two ends of the divided hyoid in expansion (hyoid expansion) (“>Fig. 51.6).
< div class='tao-gold-member'>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


