Fig 21.1 Patients often present with an adequate bone volume in the anterior as well as posterior regions of the maxilla and mandible to insert adequate number of implants with adequate size without performing any grafting procedure to provide full mouth fixed prosthesis. (A–J) Panoramic and CT scan cross-sections show adequate bone dimensions to insert adequate number of implants with ideal dimensions to support a full mouth fixed ceramic prosthesis.
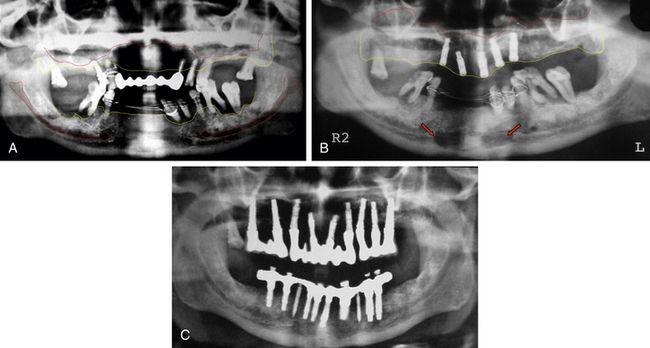
Fig 21.2 Many patients present with inadequate bone dimensions to insert adequate number of implants with adequate dimensions and thus need minor to major bone augmentation procedures to rehabilitate the patient with full mouth, implant-supported fixed prosthesis. (A) Panoramic radiograph shows inadequate bone height under the maxillary sinuses to insert implants. (B) The bilateral sinus grafting is performed using autogenous bone harvested from the mandibular symphysis (red arrows) mixed with bone substitutes to regenerate new bone dimensions in the sinuses. (C) The implants are inserted 10 months after the sinus grafting and restored after further healing period of 4 months. Thus, the case is completed in 14 months.
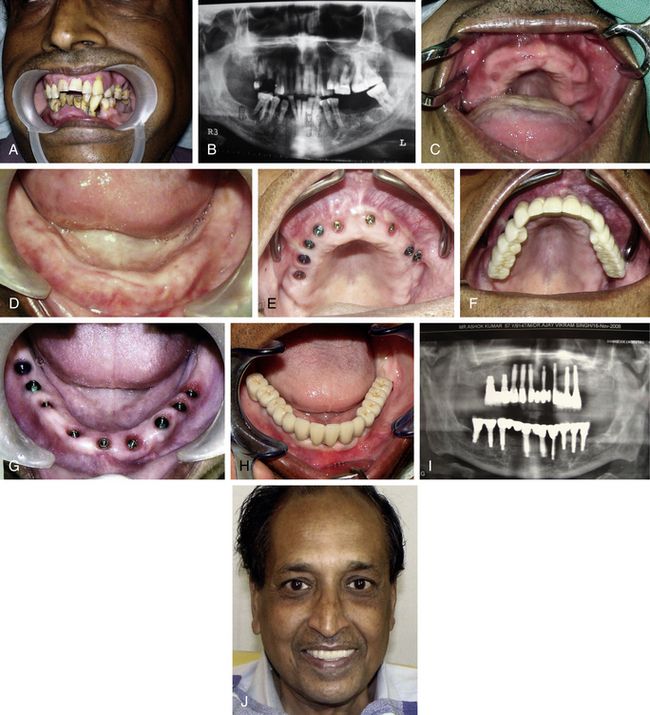
Fig 21.3 Traditional full mouth rehabilitation using implant-supported fixed ceramic prosthesis also requires placement of several implants with or without augmentation procedures. (A and B) Patient with all periodontally compromised teeth, which need extraction, and implant-supported prosthesis. (C and D) All teeth are extracted and soft relined dentures are given to the patient for 6 weeks, till all the soft tissue is healed. (E–J) Multiple implants are inserted in the upper and lower jaws to support fixed implant-supported cement-retained ceramic prosthesis.
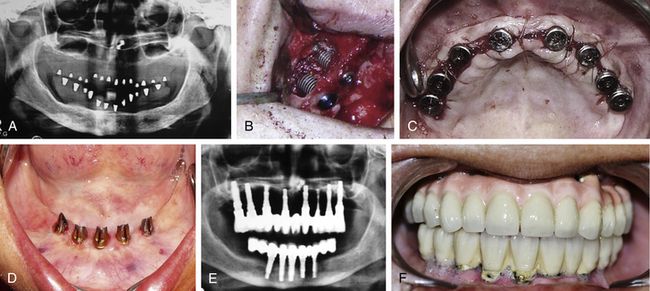
Fig 21.4 (A) Edentulous patient who has been wearing soft tissue supported dentures for more than 10 years, has lost vertical bone height in the upper and lower posterior regions. (B and C) Sinus grafting procedure is performed in posterior maxilla to insert implants in the upper full-arch. (D and E) Five implants are inserted between two mental foramina and fixed cement-retained prosthesis with distal cantilevers is fixed on lower implants. It took a complete year to give a fixed ceramic prosthesis to the patient. (F) Poor maintenance of the prosthesis by the patient lead to large amount of calculus which can be seen around the lower implants, causing various problems like frequent bleeding, soft tissue recession, and crestal bone resorption.
Disadvantages of full-arch fixed prosthesis
1. Expensive, because of the need for more implants.
2. Often needs expensive and more invasive bone augmentation procedures.
4. More specific implant placement needed.
7. More and continuous forces on the implants cannot be avoided in patients with parafunctional forces (bruxism).
8. Less support to the perioral muscles when compared to overdentures.

CASE REPORT-1
Step by step procedure for mandibular implant-supported fixed prosthesis (< ?xml:namespace prefix = "mbp" />
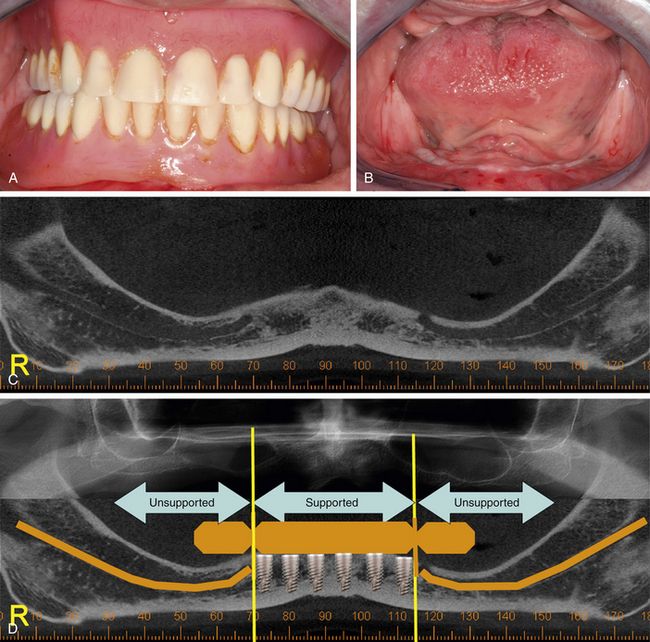
Fig 21.5 (A and B) Patient wearing soft tissue-supported dentures, complained of a retention problem with the lower denture because of age-related severe ridge resorption. The patient expressed a strong desire to have lower teeth fixed over implants. (C) The panoramic view of the mandible shows inadequate bone height above the mandibular canals to insert implants in the posterior segments. (D) Vertical bone augmentation procedures were refused by the patient, hence a fixed distal cantilevered 12-unit ceramic prosthesis, supported by 6 implants to be placed between mental foramina, is planned. Patient was advised to go for upper implant-supported ceramic prosthesis, once she was satisfied with the lower one.
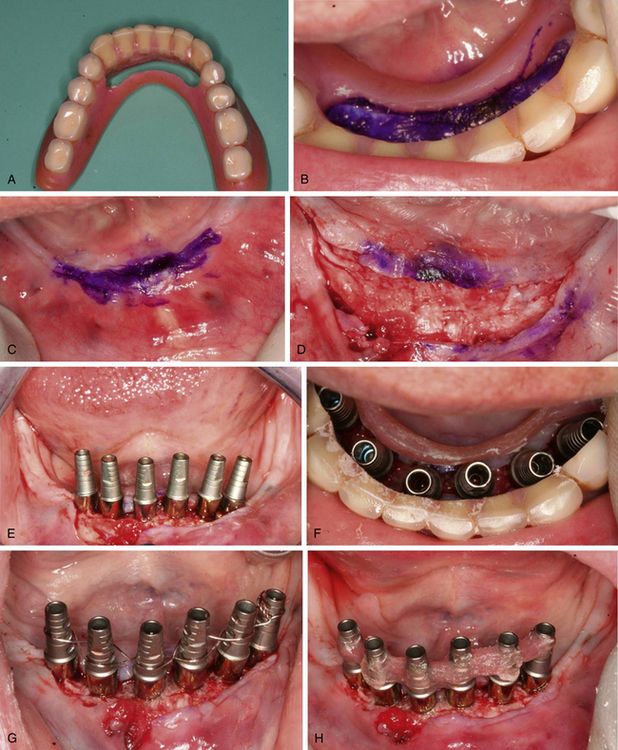
Fig 21.6 (A) Denture base is cut for prosthetically guided implant placement. (B) Denture is seated in mouth and ridge area is marked using tissue pencil. (C) Denture is removed, (D) flaps are elevated to expose the bony ridge, (E and F) and six implants are inserted between two mental foramina at the appropriate prosthetic positions. All the implants achieved adequate primary stability (more than 35 Ncm), thus an implant-supported fixed provisional prosthesis is planned to be fixed immediately on the inserted implants. (G) All the implant abutments are splinted together using a stainless steel wire, (H) which is further reinforced using the self-cure resin to firmly engage them together.

Fig 21.7 (A) Denture is passively seated in the mouth in the correct occlusion and resin is added to bond the abutments with the denture in position. (B) Once the resin gets set, the abutments along with attached denture, are unscrewed out of the mouth. (C) The resin is further added at the tissue as well as occlusal surface to fill all the peri-abutment spaces of the denture. (D) The part of the abutments occlusally emerging out of the denture has been reduced. The distal part of the denture is also reduced to limit the prosthesis up to the first molar, to minimize the cantilevering of the prosthesis. (E) Flaps are sutured and the prosthesis is screwed in the mouth. (F) Postoperative radiograph. After 3 weeks, when the soft tissue has healed, (G) prosthesis is unscrewed out from the mouth, and impression posts are inserted on top of the implants, and (H) splinted together using pattern resin.
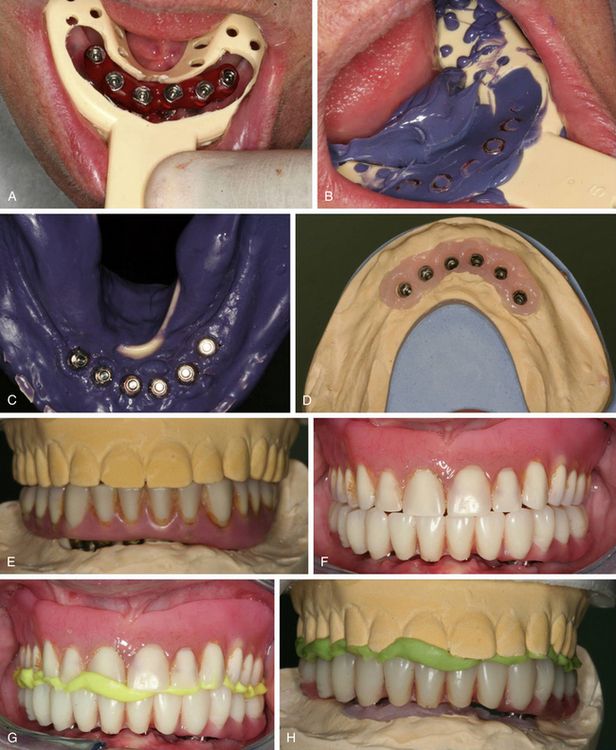
Fig 21.8 (A–C) The custom impression tray has been modified for the open tray technique and impression is made with open tray technique using polyether impression material. (D) The working cast is fabricated, and (E) denture is fixed over the cast. (F and G) A duplicate prosthesis is fabricated for the bite registration and lab purposes, and is fixed in the mouth for bite registration. (H) The working cast is rearticulated at the correct centric position.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


