Until the early 1970s, successful treatment with the Begg technique and the Tweed edgewise technique required tedious wire bending. The introduction of Andrews’ straight wire appliance changed that, and it was one of the most significant contributions in the history of orthodontics. The straight wire appliance significantly reduced the amount of wire bending and also brought along other options in treatment mechanics. Retraction of the canines with elastic chains and ligature wires became more common. Sliding mechanics in place of closing loops became the method of space closure for a significant number of clinicians. Edgewise force levels were initially used to close spaces; however, it was soon observed that lighter forces were more effective with sliding mechanics. Along with these changes, it became apparent that compensation in the appliance was needed, depending on the type of malocclusion and particularly with varying extraction sequences. Various appliance designs were developed to accommodate changes in mechanics and force levels. These modifications improved tooth positions at the end of treatment as long as the brackets were properly placed. These major changes in appliances, force levels, and treatment mechanics can be traced back to the work of Dr Lawrence Andrews and the straight wire appliances.
Highlights
- •
Until the 1970s, the Begg and Tweed edgewise techniques required tedious wire bending.
- •
Andrews’ straight wire appliance significantly reduced the need for wire bending.
- •
Undesirable side effects led to further modifications.
- •
Better appliance designs, force levels, treatment mechanics can be traced to Andrews.


This article presents a 40-year overview of our experience with treatment mechanics and contemporary appliance designs. Fortunately, due to the periodontal ligament and bone biology, teeth move in every direction. Some of these movements are positive and beneficial for the patient, and some are not. Therefore, there have been many ideas on how and how not to move teeth. Countless methods of treatment mechanics have been developed, and experience with these has led to many different appliance designs. This has been the pattern throughout the history of orthodontics. Clinicians have established their ideas on treatment mechanics and then have developed or used appliances to complement their mechanics. With these observations in mind, it is important to clarify that this article is not intended to provide criticism of what others have done with orthodontic appliances, because mechanics have led to many of their decisions. Instead, it discusses the path we chose and how mechanics have driven our appliance modifications.
Precursors to the preadjusted appliance
Before the 1970s, 2 major treatment systems were used in orthodontics: the Begg light-wire technique with the Begg appliance, and the Tweed technique with the edgewise appliance. These treatment systems were developed in response to an orthodontic philosophy of nonextraction treatment in nearly all orthodontic patients, as recommended by Edward H. Angle. Both P. Raymond Begg and Charles Tweed proposed that it was appropriate to extract teeth when crowding or protrusion was present to an extent that nonextraction treatment would lead to instability and potential periodontal breakdown. They demonstrated numerous extraction cases to support their position. Begg recommended a 3-stage approach to treatment using round wires. Multiple-loop 0.016-in round wires and light force levels were used in stage 1 for early alignment. In stage 2, teeth were tipped into the extraction sites, and spaces were closed. Finally, heavier round wires and auxiliaries were used in stage 3 to upright the teeth and correct the root positions. Orthodontists needed skill and experience to achieve good results, and the treatment method was labor intensive.
Tweed was concerned with the stability of his patients. The greatest area of concern was the mandibular anterior segment, where bone is the thinnest and multiple forces from all directions are brought to bear on these teeth. He proposed that the most stable position for the mandibular incisors was when they were positioned at 90° to the mandibular plane. Tweed believed that the most efficient and effective way to move teeth was in a bodily manner, especially in extraction patients, where the potential to tip teeth into the extraction sites was the greatest. He further believed that the most efficient force level and wire shape for bodily movement was in the 600-g range with rectangular wires. Edgewise brackets were milled (cut from larger pieces of metal). Their bases were formed at 90° angles to the tooth surface, and their rectangular slots, originally at size 0.022 in, were cut at 90° angles. Patients progressed from round wires to rectangular wires, where major tooth movements were carried out. In the early round-wire stages of treatment, horizontal in-and-out and rotational bends (first-order bends) were placed in the maxillary lateral incisors and in the maxillary and mandibular canines and molars. To aid in bodily movement, varying amounts of vertical tip bends (second-order bends) were placed. “Beauty bends” were placed in the incisor areas for tip control and esthetics. “Gable bends” were used in the canine and premolar regions to control tipping, where extractions most frequently occurred, and tipping was the greatest issue. “Tip-back bends” were used in the premolar and molar areas to control forward tooth tipping and to aid in anchorage control (needed to achieve maxillary and mandibular incisor positions). Once elastic chains became available, they were used for canine retraction in the early round-wire stages of extraction cases. Omega loops mesial to the first molars were used to “tie back” the archwires to minimize anterior tooth flaring. In rectangular wires, in addition to first- and second-order bends, torque bends (third-order bends) were placed in the incisor, premolar, and molar areas to correct the patient’s torque needs. Closing loop arches with omega loop tie-backs were used to close spaces. Although the 0.022-in slot was the most popular size during most of the edgewise era, 0.018-in slots were later introduced, with the assumption that a smaller slot and lighter wires would create lighter forces. Since forces are also based on wire deflection, this assumption was questioned by those who used the 0.022-in slot. It was a significant challenge for Tweed to achieve his goals with the edgewise brackets and labor-intensive mechanics. He met this challenge, and his treatment method significantly influenced the development of preadjusted appliances in the future.
Andrews’ straight-wire appliance
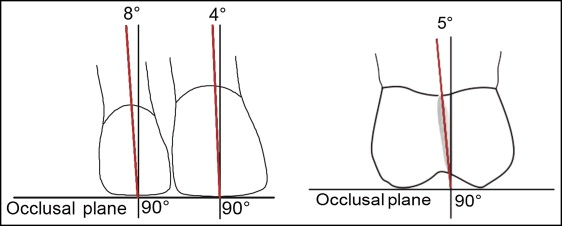
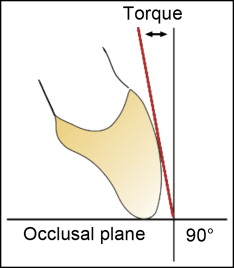
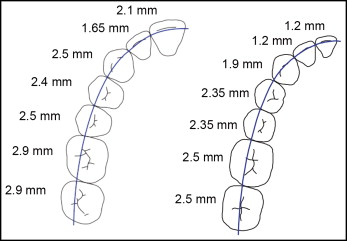
It was against this edgewise backdrop that Lawrence F. Andrews developed the first “fully programmed preadjusted” appliance. Andrews, an excellent edgewise orthodontist, thoroughly understood the nuances of edgewise treatment. He began his journey to develop the appliance by collecting 120 nonorthodontic normal models. These were models of patients whom Andrews assessed as having ideal occlusions, and who had never had orthodontic treatment. He studied these models and observed many features but found 6 features or “6 keys” that were consistent in all of the models. He published these observations in his classic article “The six keys to normal occlusion.” These keys included molar relationship, crown tip, crown torque, rotations, lack of spaces, and plane of occlusion, and they are an important part of the American Board of Orthodontics grading system used today. He then measured the in-and-out, tip, and torque values for each tooth on the models. He used 3 references to measure these values: the center of the clinical crowns, the long axis of the center of the clinical crowns, and the thickness of the clinical crowns from a designated position on the teeth to the center of the clinical crowns ( Figs 1-3 ). This allowed him to have consistent measurements on small and larger teeth. Once these data were collected, norms and standard deviations were determined. He then converted this information into a “preadjusted” appliance with tip, torque, and in-and-out values built into each bracket for each tooth. He called it the straight-wire appliance (SWA).
Andrews realized that 2 important factors were needed to develop the SWA. First, each bracket needed a “compound contoured” base, which would fit each tooth mesiodistally and occlusogingivally while positioned at the center of the clinical crown and centered on the long axis of the clinical crown. Second, if a rectangular archwire was adjusted to the shape of each model and positioned along the center of the clinical crown, each slot needed to passively accept the rectangular archwire. These 2 factors were critical to the appliance design.
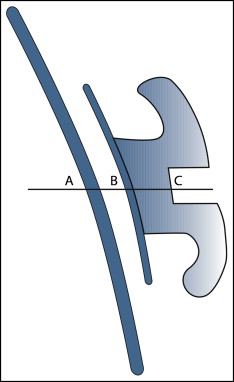
To achieve these 2 goals, Andrews realized that 3 points needed to be positioned on the same horizontal plane. These were the center of the clinical crown, the center of each bracket base, and the center of the bracket slot ( Fig 4 ). This would allow the in-and-out and torque values in the appliance to correspond with the in-and-out and torque values measured on the nonorthodontic normal models. To allow this 3-point horizontal alignment, Andrews further realized that he needed to vary the angles at the bracket bases from 90° to varying amounts of acute and obtuse angles. This resulted in a feature referred to as “torque in base,” which was patented by Andrews. This required other manufacturers that did not have the patent to place not only tip, but also torque, into the face of the brackets. In the SWA, tip was properly placed into the face of rectangular brackets, and the thickness of the brackets was determined by the in-and-out measurements on the models. The 0.022-in slot was Andrews’ choice of slot size. He decided that the best choice in manufacturing these brackets was to cast the brackets with stainless steel, similar to the casting of crowns or inlays. The difficulty with casting brackets was that stainless steel had never been cast in this manner. The temperatures to cast stainless steel were much higher than for gold. To accomplish this, he sought out engineers who determined how to carry out this process, and the brackets were constructed. This monumental effort by Andrews was one of the most significant contributions in the history of orthodontics. His work created a baseline reference for all future preadjusted appliances in the specialty.
Andrews’ straight-wire appliance
It was against this edgewise backdrop that Lawrence F. Andrews developed the first “fully programmed preadjusted” appliance. Andrews, an excellent edgewise orthodontist, thoroughly understood the nuances of edgewise treatment. He began his journey to develop the appliance by collecting 120 nonorthodontic normal models. These were models of patients whom Andrews assessed as having ideal occlusions, and who had never had orthodontic treatment. He studied these models and observed many features but found 6 features or “6 keys” that were consistent in all of the models. He published these observations in his classic article “The six keys to normal occlusion.” These keys included molar relationship, crown tip, crown torque, rotations, lack of spaces, and plane of occlusion, and they are an important part of the American Board of Orthodontics grading system used today. He then measured the in-and-out, tip, and torque values for each tooth on the models. He used 3 references to measure these values: the center of the clinical crowns, the long axis of the center of the clinical crowns, and the thickness of the clinical crowns from a designated position on the teeth to the center of the clinical crowns ( Figs 1-3 ). This allowed him to have consistent measurements on small and larger teeth. Once these data were collected, norms and standard deviations were determined. He then converted this information into a “preadjusted” appliance with tip, torque, and in-and-out values built into each bracket for each tooth. He called it the straight-wire appliance (SWA).


