Introduction
In this study, we aimed to evaluate the influence of clinical experience and the type of tooth (incisors, canines, and premolars) on the vertical accuracy of bracket placement with the Boone gauge.
Methods
For this analysis, 4 groups were defined. Group 1 was composed of undergraduate students from the dental school with no previous experience in bonding orthodontic attachments; group 2 was composed of graduate students in the dental school; group 3 consisted of orthodontists with a maximum of 5 years of clinical experience; and group 4 comprised orthodontists with more than 5 years of clinical experience. Each group included 6 participants. A typodont was simulated with a Class I crowded malocclusion that reproduced the same occlusal characteristics for all groups to be bonded. All participants were instructed to bond 0.022 × 0.028-in edgewise brackets on the labial surfaces of the maxillary and mandibular incisors, canines, and premolars at a height of 4 mm from the incisal edge or the labial cusp tip. After each bonding procedure, all teeth were photographed after being removed from the typodont and positioned in a stabilizing device adapted to a camera stand.
Results
The analyses of the variations showed that group 1 had the closest mean to 4 mm. However, this group also showed the greatest variance (0.433) ( P <0.001). The smallest variations were observed in group 2 (variance, 0.093), followed by group 4 (variance, 0.094). The comparison of the means obtained in the groups of teeth at 4 mm demonstrated that the incisors showed a statistically significant difference ( P <0.001), whereas canines ( P = 0.133) and premolars ( P = 0.913) did not.
Conclusions
Operators are prone to fail in the placement of orthodontic attachments with the Boone gauge, despite their clinical experience in orthodontics. In the comparison of the groups of teeth, the incisors showed a statistically significant difference in relation to the height suggested for bracket placement with the Boone gauge.
Highlights
- •
Incisors are related to higher bracket placement errors in orthodontics.
- •
Bracket placement failures with a Boone gauge are not related to operator experience.
- •
Free gingival-occlusal inclination disposes a positioning gauge to placement error.
A main objective of orthodontic treatment is to obtain a functional and esthetic balance between dental, skeletal, and facial structures. The placement of attachments is a critical phase of the orthodontic treatment. Failures during this step may result in difficulties during treatment, longer chair time, and inadequate final results, since the positions of these attachments on the teeth determine the final positions of the teeth.
The intensity and direction of forces are determined by the orthodontist because the details and sophistication of the orthodontic equipment cannot determine such characteristics. Therefore, excellence in the placement of orthodontic brackets is the determining factor for the correct dissipation of forces and the progression of treatment.
The consequences of the wrong vertical position of orthodontic attachments are unlevel teeth, torque alterations, changes in the labiolingual inclinations of the teeth, and alterations in arch length, compromising the teeth’s functional integrity and even causing distortions in their prescriptions. The labiolingual inclinations may be influenced by the anatomic variations on each labial surface of the tooth, by different orientations of the long axis of the root in relation to the crown of the tooth, and by the vertical position of the orthodontic attachments. A 3-mm height variation in the bracket position may lead to a 15° torque alteration.
Since there is no consensus among researchers about the ideal height for the placement of the orthodontic attachments, devices for bracket positioning that allow choosing different heights are commonly used. Although some authors have stated that brackets should be placed in the center of the clinical crown of the tooth, others have suggested different heights for the placement of these attachments.
Orthodontic positioning devices were created to determine the ideal manner to place the attachments on the tooth surface. Among the most used ones is the Boone gauge, also known as the star-like gauge, pole-like gauge, and height-bracket position gauge.
Notwithstanding all of the technological developments, the correct vertical position of the orthodontic attachment during bonding procedures can be influenced by individual interferences and the anatomic characteristics of each tooth. The inherent human limitation on the determination of the height for the placement of orthodontic attachments requires compensatory bends for finishing the orthodontic treatment.
In this study, we aimed to evaluate the influence of clinical experience and the type of tooth (incisors, canines, and premolars) on the vertical accuracy of bracket placement with the Boone gauge.
Material and methods
For this analysis, 4 groups were defined. Group 1 was composed of undergraduate students in the dental school at Juiz de Fora Federal University in Brazil who had no previous experience in bonding orthodontic attachments. Group 2 was composed of graduate students in the dental school. Group 3 consisted of orthodontists with a maximum of 5 years of clinical experience. Group 4 comprised orthodontists with more than 5 years of clinical experience. Each group included 6 participants, totaling 24 subjects ( Table I ).
| Group | Participants | Number of participants | Number of teeth |
|---|---|---|---|
| 1 | Undergraduate students | 6 | 120 |
| 2 | Graduate students | 6 | 120 |
| 3 | Orthodontists with a maximum of 5 years of clinical experience | 6 | 120 |
| 4 | Orthodontists with more than 5 years of clinical experience | 6 | 120 |
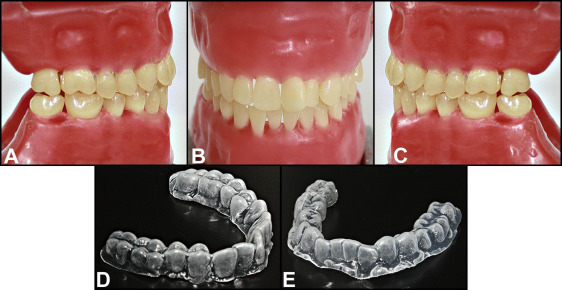
A typodont was simulated with a Class I crowded malocclusion with the aid of an acetate impression tray, which reproduced the same occlusal characteristics for all groups of participants ( Fig 1 ). The teeth were positioned so that they did not interfere with the use of the Boone gauge and the correct position of the brackets.
With the objective of standardization, an educational video about bonding procedures was shown to each subject before bonding. All participants were instructed to bond 0.022 × 0.028-in edgewise brackets (380-0021; American Orthodontics, Sheboygan, Wis) on the labial surfaces of the maxillary and mandibular incisors, canines, and premolars (20 bonded teeth per subject), at a height of 4 mm from the incisal edge or the labial cusp tip, with the typodont simulating working clinical conditions. To determine the height position of the bracket, we used a Boone gauge (010-010, American Orthodontics). The operators were given procedure gloves, a Hollenback carver (CVHL1/29; Hu-Friedy, Chicago, Ill), an exploring probe (XP23/PH6; Hu-Friedy), a clinical mirror (M8H; Hu-Friedy), a cotton tweezer (DPU17; Hu-Friedy), and an orthodontic tweezer (678-212; Hu-Friedy). Brackets were bonded with a light-cured composite resin (712-036, Transbond XT; 3M Unitek, Monrovia, Calif) for 5 seconds. Since the teeth were made of plastic and shear bond strength was not under evaluation, no acid etching was performed, and no bonding agent was applied. After each bonding procedure, all teeth were photographed after being removed from the typodont and positioned in a stabilizing device adapted to a camera stand. This stabilizing device had holes molded with self-polymerized acrylic resin (Coldpac Ortho Resin; Yates Motloid, Chicago, Ill) that positioned the teeth with their mesial surfaces parallel and toward the camera lens, standardizing the position of the teeth in all photographs. An EOS XSi camera of 13 megapixels (2756B001; Canon, Oita, Kyushu, Japan) with a macro lens of 100 mm, shutter speed of 1/100 second, and aperture of f/2.8 ( Fig 2 ) positioned 20 cm from the stabilizing device was used. A millimetric ruler (CLR6; Hu-Friedy) was inserted in the photographed field to determine the real dimensions of the images from the digital ones using the software for Mac OS (version 6.1, Keynote for Mac; Apple, Cupertino, Calif).

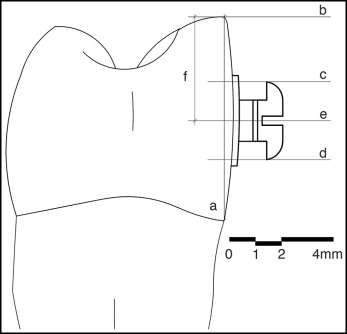
The determination of the representative plane of the labial surface of the teeth was done with the mesial view using the union of the most anterior point of the cementoenamel junction and the most incisal point of the tooth ( Fig 3 , A ). For the determination of the height of the bonded brackets, the following lines perpendicular to the labial plane were traced: tangent line to the most incisal point (or labial cusp tip) ( line b , Fig 3 ); tangent line to the occlusal border of the bracket wings ( line c , Fig 3 ); tangent line to the cervical border of the bracket wings ( line d , Fig 3 ); and equidistant line to lines c and d ( Fig 3 ), representing the geometric center of the bracket slot ( line e , Fig 3 ). The bonding distance corresponded to the distance between the points in which lines b and e intercepted the representative plane of the labial face of the tooth ( segment f , Fig 3 ).