This chapter provides an overview of speech characteristics, evaluation techniques, and management approaches for the patient with repaired cleft palate with or without cleft lip. The intended audience is oral and maxillofacial surgeons, speech-language pathologists (SLPs), and other health care professionals who have basic knowledge of both cleft conditions and the anatomy and physiology of the vocal tract. The chapter begins with a discussion of the multiple causes of speech disorders among patients with cleft palate. Multiple causes are emphasized, as most textbooks tend to focus on velopharyngeal dysfunction as the cause of speech disorders and neglect the contribution of other structural factors. Next, core speech characteristics of individuals with repaired cleft palate and velopharyngeal dysfunction are described. Both perceptual and instrumental assessment techniques of speech and velopharyngeal function are then reviewed. The chapter concludes with an overview of the role of secondary surgery, prosthetics, and behavioral approaches to treatment.
ETIOLOGY OF SPEECH DISORDERS IN INDIVIDUALS WITH CLEFT PALATE
Although SLPs have traditionally focused on inadequate function of the velopharyngeal mechanism as the primary cause of speech problems in individuals with cleft palate, other factors are also involved. It is well known that alveolar and dental anomalies associated with clefts of the primary palate contribute to speech disorders. In addition, because eustachian tube dysfunction and otitis media are almost universal in children with cleft palate, the deleterious effects of conductive hearing loss on speech acquisition must be considered. Finally, it must be emphasized that children born with cleft palate are not immune from developing other speech problems during childhood such as phonologic disorders, apraxia of speech, and stuttering. Relative to the last, Dalston and co-workers, however, reported that for unknown reasons, the prevalence of stuttering among children with cleft palate is actually lower than expected. Regardless, the point to be made is that children with cleft palate are a challenge relative to the diagnosis of speech problems that might result from multiple causes. Clearly, differential diagnosis of the underlying cause of speech problems is essential if appropriate treatment recommendations are to be made.
VELOPHARYNGEAL DYSFUNCTION
The primary goal of surgical repair of clefts of the secondary palate is to restore the muscular integrity of the velopharyngeal structures to enable normal speech development. Although the timing of palate repair varies greatly across institutions, current consensus for initial palate surgery of infants in the United States appears to be 9 to 12 months of age. If a cleft of the primary palate is involved, definitive correction of the alveolar defect is delayed until the child is approximately 8 to 9 years of age and is in mixed dentition. Typically, review of studies indicates that the success rate for surgical repair of clefts involving the secondary palate is appropriately 70-80%.
For the child born without cleft palate, we expect that by 3 to 4 years of age he or she will naturally acquire vowels, nasal consonants, and stop-plosive consonants. In English, stop-plosives are articulated primarily at three locations in the oral cavity: bilabial for /p/ and /b/, lingual-alveolar for /t/ and /d/, and lingual-velar for /k/ and /g/ ( Table 39-1 ). By the time a child is 7 to 8 years of age, we expect that the en- to 4 year-old child born with a cleft of the secondary palate in whom surgery was not successful, the phonetic inventory may consist of only vowels, nasal consonants, and vowel-like consonants (e.g., /w/ and /j/) that do not require the buildup of intraoral air pressure. In addition, as described later, some children may develop pharyngeal and/or glottal articulations in an attempt to compensate for velopharyngeal dysfunction. Velopharyngeal dysfunction will also affect production of fricative and affricate consonants in older children. Table 39-1 highlights the stop, fricative, and affricate consonants that are likely to be affected by velopharyngeal dysfunction. As illustrated, inadequate velopharyngeal function has the potential to affect a majority of English consonants.
| Labial | Labiodental | Interdental | Alveolar | Palatal | Velar | Glottal | |
|---|---|---|---|---|---|---|---|
| Stops | P b | t d | k g | — | |||
| Nasals | m | n | 3 | ||||
| Fricatives | f V | > ? | s z | B C | h | ||
| Affricates | tB, | ||||||
| Laterals | 1 | r | |||||
| Glides | w | j |
In addition to congenital clefts of the secondary palate, velopharyngeal dysfunction may occur in children because of congenitally deep nasopharynx; obstructing tonsils and/or adenoids; and neuromotor problems such as dysarthria and/or apraxia. Diagnosis and management decisions that involve children with repaired cleft palate, therefore, need to take possible co-existing factors into consideration.
DENTAL AND ALVEOLAR ANOMALIES
When clefts involve the primary palate, structural anomalies involving the teeth and alveolar ridge are likely to occur. Missing and/or supernumerary teeth are often found in and around the cleft site. Maxillary collapse and resulting posterior crossbites are common. Oral-nasal fistula may also occur, especially during maxillary expansion as part of orthodontic treatment. Even in cases of isolated clefts of the secondary palate, there may be alveolar and/or palatal morphologic anomalies that occur as the result of growth restriction due to surgical repair. In addition, clefts of the secondary palate are often associated with syndromes and/or sequences such as Pierre-Robin, which may directly cause dental malocclusion. Although alveolar and dental anomalies have long been noted to affect speech production, surprisingly, the extent of the impact of these structural problems on speech intelligibility has not been systematically investigated. Table 39-2 highlights the consonants that are likely to be affected by alveolar and dental anomalies. As illustrated, a majority of consonants are produced by bringing the lips and tongue into contact with the teeth, alveolar ridge, and hard palate.
| Labial | Labiodental | Interdental | Alveolar | Palatal | Velar | Glottal | |
|---|---|---|---|---|---|---|---|
| Stops | P b | t d | k g | — | |||
| Nasals | m | n | 3 | ||||
| Fricatives | f V | > ? | s z | B C | h | ||
| Affricates | tB, | ||||||
| Laterals | 1 | r | |||||
| Glides | w | j |
OTHER CAUSES
Because of the disruption of velar morphology caused by palatal clefting, infants with cleft palate are prone to a sequence of eustachian tube dysfunction, development of otitis media with effusion (OME), and mild to moderate conductive hearing loss. Indeed, the prevalence of OME in children with cleft palate has been reported to be more than 95%. Roberts and Clarke-Klein identified three ways in which persistent OME might disrupt normal development of speech and language. First, reduced hearing acuity might result in inaccurate encoding of perceptual information. Second, prolonged hearing reduction might impair a child’s ability to discriminate linguistic information, characterized by low perceptual saliency (e.g., morphophonemic markers). Third, illnesses associated with OME might “restrict or alter the child’s interactions with people and objects in the environment,” thus reducing available opportunities for speech and language learning. Although these disruptions have obvious face validity, available research has indicated an equivocal relationship between the occurrence of early conductive hearing loss as a consequence of OME and subsequent development of speech and language in children without cleft palate.
In contrast to children without cleft palate, only a few studies have investigated the impact of conductive hearing loss on speech acquisition in children with cleft palate. Hubbard, in a retrospective study, reported that articulation scores were better in a group of children with cleft palate who received early and aggressive ear care as compared with a group of children with cleft palate who did not receive early ear care. Broen and colleagues studied infants with and without cleft palate longitudinally to age 30 months. These investigators reported that hearing levels of the infants accounted for significant differences on cognitive and developmental measures between the cleft and noncleft groups. Clearly, additional research is needed to gauge the impact of early hearing loss as a result of OME in children with repaired cleft palate.
Finally, we know that approximately 6-10% of children without cleft palate will require speech therapy for idiopathic or functional articulation disorders. In addition, developmental neuromotor disorders such as apraxia of speech may occur in children and can dramatically reduce speech intelligibility. Obviously, children born with cleft palate are not immune to such speech disorders. Indeed, relative to children with velopharyngeal dysfunction who also have velocardiofacial syndrome, Kummer and colleagues (2007) reported an increased prevalence of apraxia of speech.
SPEECH CHARACTERISTICS OF INDIVIDUALS WITH CLEFT PALATE
After initial palate repair, approximately 20-30% of children will exhibit speech characteristics that reflect inadequate velopharyngeal function. These characteristics include hypernasal resonance during vowel production, nasal air emission (visible and/or audible) during consonant production, and reduced oral air pressure during consonant production. These speech characteristics are often referred to as obligatory symptoms because they naturally occur in the presence of inappropriate oral-nasal coupling. In addition, children with velopharyngeal dysfunction may alter tongue placement for articulation of consonants. These misarticulations are referred to as compensatory behaviors in that they are learned in response to inadequate velopharyngeal closure.
RESONANCE IMBALANCE
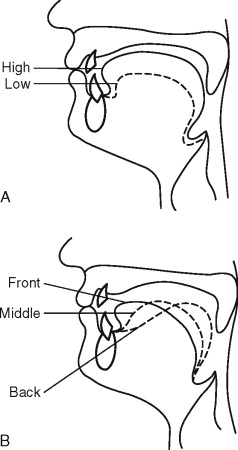
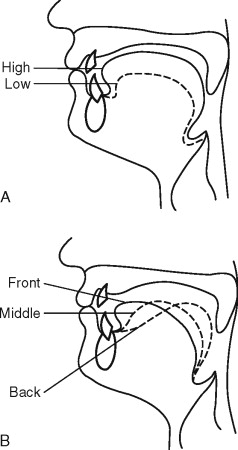
Resonance is a complex perceptual phenomenon associated with vowels and voiced consonants that occurs because of acoustic excitation of the air-filled cavities of the upper vocal tract, primarily the pharynx, oral cavity, and nasal passages. In English, speakers without cleft palate will produce vowels and oral consonants with nearly complete separation of the oral and nasal cavities as illustrated in Figure 39-1 . This is accomplished by elevation and retraction of the soft palate and sphincter-like closure of the upper pharyngeal walls. The primary resonating cavities, therefore, are the pharynx and mouth. During production of the nasal consonants (/m/, /n/, and /3/) and vowels that precede or follow a nasal consonant, the soft palate will relax and lower to some degree. Nasal resonance, therefore, will be perceived during these speech sounds. The primary determinants of normal nasal resonance during nasal consonants and adjacent vowels are (1) the physical characteristics of the nasal cavities such as volume and cross-sectional area, and (2) the temporal extent of velar lowering before and after nasal consonants (i.e., anticipatory and carryover nasalization), respectively. In addition, some normal nasal resonance may occur during production of nonnasalized vowels and voiced oral consonants owing to the extent that the air mass in the nasal cavity is excited even in the presence of complete velopharyngeal closure. This phenomenon—sometimes referred to as sympathetic vibration —is determined by a complex interaction between the fundamental frequency of the speaker and the physical characteristics (mass and stiffness) of the elevated soft palate.
For a speaker with repaired cleft palate who has incomplete velopharyngeal closure, inappropriate acoustic coupling of the oral and nasal cavities will occur and result in a hypernasal resonance imbalance during production of vowels and voiced, nonnasal consonants. The degree of the perceived hypernasality will be determined primarily, but not exclusively, by the physical extent of the coupling of the oral and nasal cavities. As noted previously, both temporal characteristics of nasalization and physical characteristics of the velum also may contribute to hypernasality. Indeed, even if a speaker with repaired cleft palate achieves complete velopharyngeal closure, it is possible that resonance may be hypernasal owing to physical changes in the velum caused by surgery (e.g., increased stiffness due to scarring).
Finally, it must be noted that some speakers with repaired cleft palate may exhibit primarily hyponasality or mixed hypernasality and hyponasality. Hyponasality will occur during production of nasal consonants and adjacent vowels when the nasal cavities are obstructed. The location of the obstruction may be posterior and include hypertrophied tonsils and/or adenoids or anterior and include deviated septum, hypertrophied turbinates, and/or a collapsed nasal vestibule.
NASAL AIR EMISSION
Nasal air emission (or escape) is distinct from hypernasality both in perceptual features and affected speech sounds. Nasal escape refers to the visible or audible transmission of air that accompanies stop-plosives and/or continuant consonants. Audible nasal escape may be brief when it accompanies stop-plosives (confined to the closure phase of the consonant) or relatively prolonged when it accompanies continuants such as /s/. Although audible nasal escape may occur during both voiced and voiceless consonants, it is most salient during production of voiceless sounds. This occurs because voiceless sounds are typically produced with higher levels of intraoral air pressure than voiced sounds. Unlike hypernasality, the presence of nasal air escape always implies the direct physical coupling of the oral and nasal cavities at some location (i.e., at either the velopharynx and/or a fistula at some point along the palate). Although hypernasality and nasal escape may co-occur, each may occur without the other.
Because of the complex nature of audible nasal escape and anatomic variability among speakers, it is not unexpected that there have been numerous and at times somewhat confusing descriptions of nasal air emission reported in the literature. Peterson-Falzone and co-workers described “audible” nasal air escape as the sound that is produced when one “forcefully exhales through the nose.” They further describe a severe form of audible nasal air emission that they term “turbulent” and attribute to increased “intranasal” resistance. Kummer and co-workers have referred to a type of audible nasal emission that they call “nasal rustle” and attribute to a small velopharyngeal gap. The nasal rustle appears to be similar both in perceptual and physiologic features as the “posterior nasal fricative” described by Trost. According to Trost, the posterior nasal fricative is characterized by turbulent nasal airflow that is generated by a small velopharyngeal opening, perhaps in conjunction with lingual assistance. She suggests that the posterior nasal fricative is more accurately described as a “nasopharyngeal fricative.” Regardless of the terms used, Kummer makes the excellent point that clinicians need to be aware that perceptual severity does not necessarily translate into physiologic severity when audible nasal escape is described —that is, for a given effort level, a smaller velopharyngeal (or palatal) opening will generate greater turbulence than a larger opening.
Finally, audible nasal air emission may occur in the presence of normal velopharyngeal closure as a learned misarticulation that mimics velopharyngeal inadequacy. This is often referred to as phoneme-specific nasal emission (PSNE). The distinctive perceptual quality of PSNE has been variously described as a nasal snort, posterior nasal fricative, and/or nasal rustle. The defining physiologic characteristic of PSNE, however, appears to be the simultaneous production of both an oral stop and posterior nasal fricative as a substitution for any of the fricative, sibilant, and/or affricate sounds. During production of stop-plosive sounds, velopharyngeal closure is complete. Because PSNE occurs in the presence of normal velopharyngeal closure for stop-plosives, it should logically be considered a learned phonologic error; therefore behavioral speech therapy, not surgery, is the treatment option. Zajac provides a discussion of the possible causes of PSNE and audio examples from children both with and without cleft palate. Behavioral techniques to eliminate PSNE are discussed later.
REDUCED INTRAORAL AIR PRESSURE
When velopharyngeal inadequacy exists, not only will nasal air escape occur during the closure phase of stop consonants, but the oral release burst during the plosive phase will be reduced in intensity owing to the loss of air pressure through the nose. In severe cases, an oral stop may sound more like a nasal consonant (e.g., “bat” may sound like “mat”).
ARTICULATION AND INTELLIGIBILITY
The prevalence of articulation errors in children with repaired cleft palate is high. Based on a review of the literature, Peterson-Falzone and co-workers concluded that approximately 75% of preschool children with repaired palate exhibit some type of articulation disorder. Estimates were as high as 90% in some studies. Given that multiple causes may be involved, these findings should not be surprising. As a comparison, the overall prevalence of functional articulation disorders among children without cleft palate is generally estimated to be 6-10%.
Children with cleft palate and velopharyngeal dysfunction have been described to exhibit a variety of compensatory misarticulations. As noted by Peterson-Falzone and colleagues (2001), compensatory articulations were historically considered to consist of glottal stop and pharyngeal fricative substitutions for oral consonants. A shift in articulatory constriction to a location inferior to the velopharyngeal sphincter was considered to occur in response to velopharyngeal inadequacy in order to preserve manner of production. Philips and Kent succinctly defined compensatory articulations as:
. . . behaviors that are thought to be learned and habituated [automatized] for productions of speech sounds when, due to VPI, normal productions cannot be achieved.
Given that velopharyngeal inadequacy results in an obligatory reduction in oral air pressure associated with stop consonants, it is not surprising that glottal substitutions may occur. Sherman and colleagues reported that children with cleft palate primarily substituted glottal stops for voiceless stops—which require greater oral air pressure than voiced stops.
In addition to “gross” compensatory errors such as glottal stops and/or pharyngeal fricatives, there are additional articulations typical of speakers with repaired cleft palate. Using both perceptual and radiographic techniques, Trost described the middorsum palatal stop, the posterior nasal fricative, and the pharyngeal stop. The middorsum palatal stop was described as a substitution for alveolar and/or velar stops. It is produced with the dorsum of the tongue making contact with the palate in approximately the location for production of /j/. Perceptually, it was described as a cross between /t/ and /k/ or between /d/ and /g/, depending on voicing. The posterior nasal fricative was identified as a substitution for sibilant sounds. As noted earlier, it is produced by generating turbulence through a small velopharyngeal constriction, perhaps with lingual assistance to help reduce gap size. The pharyngeal stop was identified as a substitution for velar stops /k/ and /g/. It is produced with the base of the tongue making contact against the posterior pharyngeal wall.
Because the middorsum palatal stop is produced in a location that is anterior to the velopharyngeal sphincter, it is problematic to ascribe its function as a compensatory response to velopharyngeal inadequacy. One previous report noted the frequent co-occurrence of anterior oronasal fistulas (ONFs) and middorsum palatal stops in children with repaired cleft lip and palate. Accordingly, the authors attributed the occurrence of the middorsum palatal stop to “anterior palatal defects.” Similarly, Kummer in 2001 stated that middorsum palatal stops might occur in response to malocclusion and/or dental crowding in the oral cavity, two frequent consequences of unrepaired alveolar clefts. Indeed, Okazaki reported that palatalized articulations were associated with narrowing and shortening of the anterior palate.
Whereas several investigators have suggested that the middorsum palatal stop is a frequently occurring misarticulation in children with cleft palate, its affect on speech intelligibility is largely unknown. Both trained and untrained listeners cannot consistently identify middorsum palatal stops as distinct from examples of /t/ and /k/ produced by children with repaired cleft palate. Although this is not an intelligibility task, middorsum palatal stops “may reduce the intelligibility of the individual’s speech by neutralizing the place contrast.”
Although articulation and intelligibility are often used as synonymous terms, intelligibility as a construct supersedes articulation. Kent has defined intelligibility as “the degree to which the speaker’s intended message is recovered by the listener.” Therefore intelligibility is dependent on the speaker, the situation, and the listener. Many of the early studies that investigated intelligibility in children with repaired cleft palate employed transcription or write-down techniques. In general, these studies indicated clear differences in intelligibility between subjects with and without cleft palate, a tendency for articulation and intelligibility scores to be correlated (especially errors involving stop consonants), and a tendency for intelligibility and velopharyngeal function to be correlated.
VOCAL DYSFUNCTION
Voice disorders in individuals with clefts of the palate are often reported in the literature. Hoarse vocal quality, reduced loudness, deviant and/or restricted pitch range, and tense or strained qualities are some of the commonly observed voice aberrations. These studies have also reported a high prevalence of voice disorders among individuals with cleft palate as compared with speakers without cleft palate. McWilliams and co-workers used nasoendoscopy to examine 32 children with repaired cleft palate who had hoarse vocal quality. These investigators reported that 72% of the children exhibited vocal fold nodules. Marks and co-workers reported that perceptual symptoms of dysphonia were evident in 34% of 102 speakers who were evaluated for suspected velopharyngeal dysfunction. Similarly, D’Antonio reported that 41% of 85 speakers with velopharyngeal dysfunction exhibited either perceptual symptoms of dysphonia and/or laryngeal anomalies. As a comparison, voice disorders typically occur in no more than 6% of the general population.
The high prevalence of voice disorders among speakers with velopharyngeal dysfunction is often attributed to compensatory changes in respiratory and/or laryngeal behaviors. Because nasalization of sound results in attenuation of acoustic energy, a speaker with inappropriate oral-nasal coupling will have to increase intensity to achieve a given level of loudness. One way to increase intensity is to use increased laryngeal resistance during voicing. The available evidence relative to laryngeal resistance among speakers with cleft palate, however, is equivocal. Whereas Zajac reported similar levels of laryngeal resistance in children with and without cleft palate, a study performed by Guyette reported that children with cleft palate and incomplete velopharyngeal closure exhibited higher levels of laryngeal resistance than children with cleft palate and complete velopharyngeal closure.
Some speakers with velopharyngeal dysfunction may actually reduce loudness. McWilliams refers to this phenomenon as “soft voice syndrome” and suggest that it is an attempt to mask perceptual symptoms of hypernasality and/or nasal air escape. Finally, clinicians should also be aware that vocal hoarseness will effectively mask hypernasality in many patients with repaired cleft palate. Careful attention, therefore, should be paid to patients with hoarseness.
SPEECH CHARACTERISTICS OF INDIVIDUALS WITH CLEFT PALATE
After initial palate repair, approximately 20-30% of children will exhibit speech characteristics that reflect inadequate velopharyngeal function. These characteristics include hypernasal resonance during vowel production, nasal air emission (visible and/or audible) during consonant production, and reduced oral air pressure during consonant production. These speech characteristics are often referred to as obligatory symptoms because they naturally occur in the presence of inappropriate oral-nasal coupling. In addition, children with velopharyngeal dysfunction may alter tongue placement for articulation of consonants. These misarticulations are referred to as compensatory behaviors in that they are learned in response to inadequate velopharyngeal closure.
RESONANCE IMBALANCE
Resonance is a complex perceptual phenomenon associated with vowels and voiced consonants that occurs because of acoustic excitation of the air-filled cavities of the upper vocal tract, primarily the pharynx, oral cavity, and nasal passages. In English, speakers without cleft palate will produce vowels and oral consonants with nearly complete separation of the oral and nasal cavities as illustrated in Figure 39-1 . This is accomplished by elevation and retraction of the soft palate and sphincter-like closure of the upper pharyngeal walls. The primary resonating cavities, therefore, are the pharynx and mouth. During production of the nasal consonants (/m/, /n/, and /3/) and vowels that precede or follow a nasal consonant, the soft palate will relax and lower to some degree. Nasal resonance, therefore, will be perceived during these speech sounds. The primary determinants of normal nasal resonance during nasal consonants and adjacent vowels are (1) the physical characteristics of the nasal cavities such as volume and cross-sectional area, and (2) the temporal extent of velar lowering before and after nasal consonants (i.e., anticipatory and carryover nasalization), respectively. In addition, some normal nasal resonance may occur during production of nonnasalized vowels and voiced oral consonants owing to the extent that the air mass in the nasal cavity is excited even in the presence of complete velopharyngeal closure. This phenomenon—sometimes referred to as sympathetic vibration —is determined by a complex interaction between the fundamental frequency of the speaker and the physical characteristics (mass and stiffness) of the elevated soft palate.
For a speaker with repaired cleft palate who has incomplete velopharyngeal closure, inappropriate acoustic coupling of the oral and nasal cavities will occur and result in a hypernasal resonance imbalance during production of vowels and voiced, nonnasal consonants. The degree of the perceived hypernasality will be determined primarily, but not exclusively, by the physical extent of the coupling of the oral and nasal cavities. As noted previously, both temporal characteristics of nasalization and physical characteristics of the velum also may contribute to hypernasality. Indeed, even if a speaker with repaired cleft palate achieves complete velopharyngeal closure, it is possible that resonance may be hypernasal owing to physical changes in the velum caused by surgery (e.g., increased stiffness due to scarring).
Finally, it must be noted that some speakers with repaired cleft palate may exhibit primarily hyponasality or mixed hypernasality and hyponasality. Hyponasality will occur during production of nasal consonants and adjacent vowels when the nasal cavities are obstructed. The location of the obstruction may be posterior and include hypertrophied tonsils and/or adenoids or anterior and include deviated septum, hypertrophied turbinates, and/or a collapsed nasal vestibule.
NASAL AIR EMISSION
Nasal air emission (or escape) is distinct from hypernasality both in perceptual features and affected speech sounds. Nasal escape refers to the visible or audible transmission of air that accompanies stop-plosives and/or continuant consonants. Audible nasal escape may be brief when it accompanies stop-plosives (confined to the closure phase of the consonant) or relatively prolonged when it accompanies continuants such as /s/. Although audible nasal escape may occur during both voiced and voiceless consonants, it is most salient during production of voiceless sounds. This occurs because voiceless sounds are typically produced with higher levels of intraoral air pressure than voiced sounds. Unlike hypernasality, the presence of nasal air escape always implies the direct physical coupling of the oral and nasal cavities at some location (i.e., at either the velopharynx and/or a fistula at some point along the palate). Although hypernasality and nasal escape may co-occur, each may occur without the other.
Because of the complex nature of audible nasal escape and anatomic variability among speakers, it is not unexpected that there have been numerous and at times somewhat confusing descriptions of nasal air emission reported in the literature. Peterson-Falzone and co-workers described “audible” nasal air escape as the sound that is produced when one “forcefully exhales through the nose.” They further describe a severe form of audible nasal air emission that they term “turbulent” and attribute to increased “intranasal” resistance. Kummer and co-workers have referred to a type of audible nasal emission that they call “nasal rustle” and attribute to a small velopharyngeal gap. The nasal rustle appears to be similar both in perceptual and physiologic features as the “posterior nasal fricative” described by Trost. According to Trost, the posterior nasal fricative is characterized by turbulent nasal airflow that is generated by a small velopharyngeal opening, perhaps in conjunction with lingual assistance. She suggests that the posterior nasal fricative is more accurately described as a “nasopharyngeal fricative.” Regardless of the terms used, Kummer makes the excellent point that clinicians need to be aware that perceptual severity does not necessarily translate into physiologic severity when audible nasal escape is described —that is, for a given effort level, a smaller velopharyngeal (or palatal) opening will generate greater turbulence than a larger opening.
Finally, audible nasal air emission may occur in the presence of normal velopharyngeal closure as a learned misarticulation that mimics velopharyngeal inadequacy. This is often referred to as phoneme-specific nasal emission (PSNE). The distinctive perceptual quality of PSNE has been variously described as a nasal snort, posterior nasal fricative, and/or nasal rustle. The defining physiologic characteristic of PSNE, however, appears to be the simultaneous production of both an oral stop and posterior nasal fricative as a substitution for any of the fricative, sibilant, and/or affricate sounds. During production of stop-plosive sounds, velopharyngeal closure is complete. Because PSNE occurs in the presence of normal velopharyngeal closure for stop-plosives, it should logically be considered a learned phonologic error; therefore behavioral speech therapy, not surgery, is the treatment option. Zajac provides a discussion of the possible causes of PSNE and audio examples from children both with and without cleft palate. Behavioral techniques to eliminate PSNE are discussed later.
REDUCED INTRAORAL AIR PRESSURE
When velopharyngeal inadequacy exists, not only will nasal air escape occur during the closure phase of stop consonants, but the oral release burst during the plosive phase will be reduced in intensity owing to the loss of air pressure through the nose. In severe cases, an oral stop may sound more like a nasal consonant (e.g., “bat” may sound like “mat”).
ARTICULATION AND INTELLIGIBILITY
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


