History of the Procedure
Surgical management of oral cysts was described as early as 1892 by Partsch and involved the intraoral exposure of the cyst lining (marsupialization), which came to be termed the Partsch I procedure. Because the Partsch I procedure frequently led to inadequate cyst removal and complications in the pre-antibiotic era, Partsch described the Partsch II procedure (enucleation) in 1910. Dowsett and Wassmund further developed the technique, thereby improving access for complete enucleation of the cyst through a wide intraoral osteotomy. Surgical techniques continued to improve over the decades, and the incidence of recurrence and infection subsequently declined. As the distinct benign pathologic processes of the oral and maxillofacial region became more clearly defined, it became more evident that the enucleation and curettage method was a primary choice for the initial definitive management of a majority of these lesions. For example, the keratocystic odontogenic tumor (KOT) has a high rate of recurrence, and the addition of chemical curettage, in addition to physical curettage, with enucleation had been shown to significantly decrease or eliminate the recurrence rate. The development of chemical curettage had also progressed with the utilization of Carnoy’s solution and liquid nitrogen as methods that have shown some success in decreasing recurrence rates of some lesions.
History of the Procedure
Surgical management of oral cysts was described as early as 1892 by Partsch and involved the intraoral exposure of the cyst lining (marsupialization), which came to be termed the Partsch I procedure. Because the Partsch I procedure frequently led to inadequate cyst removal and complications in the pre-antibiotic era, Partsch described the Partsch II procedure (enucleation) in 1910. Dowsett and Wassmund further developed the technique, thereby improving access for complete enucleation of the cyst through a wide intraoral osteotomy. Surgical techniques continued to improve over the decades, and the incidence of recurrence and infection subsequently declined. As the distinct benign pathologic processes of the oral and maxillofacial region became more clearly defined, it became more evident that the enucleation and curettage method was a primary choice for the initial definitive management of a majority of these lesions. For example, the keratocystic odontogenic tumor (KOT) has a high rate of recurrence, and the addition of chemical curettage, in addition to physical curettage, with enucleation had been shown to significantly decrease or eliminate the recurrence rate. The development of chemical curettage had also progressed with the utilization of Carnoy’s solution and liquid nitrogen as methods that have shown some success in decreasing recurrence rates of some lesions.
Indications for the Use of the Procedure
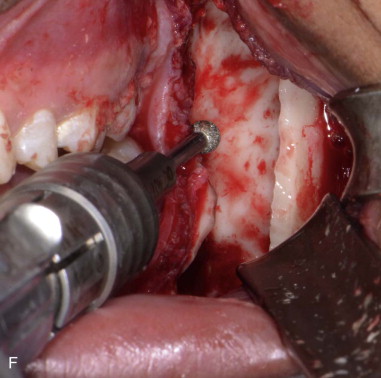
Enucleation is the surgical treatment of benign pathology that involves the complete removal of the entity. It is the procedure of choice for removal of most cysts and other benign pathology of the oral and maxillofacial region that are anatomically distinct from the surrounding tissue and amenable to this type of therapy. Physical or chemical curettage may be added to the enucleation procedure in certain pathologies that require additional removal of surrounding bone to help ensure complete removal and to decrease the persistence of the lesion. Curettage may be completed with a sharp curette or a round diamond bur with copious cool irrigation to remove 1 to 2 mm of bone and any pathology remnants. Meticulous technique in the procedure of enucleation and curettage is particularly important in the surgical management of lesions that tend to have high recurrence or persistence rates, such as the keratocystic odontogenic tumor. In this situation, the addition of Carnoy’s solution to curettage or peripheral ostectomy has been shown to be more effective in decreasing the recurrence rate than are the enucleation procedures alone. Liquid nitrogen has also been used for chemical curettage with some success in the management of the luminal and intraluminal subtypes of ameloblastoma. Enucleation and curettage may also be indicated as a second procedure in lesions that have persisted following an initial procedure of enucleation and curettage.
Simple enucleation and curettage may be indicated for unicystic ameloblastomas of the luminal and intraluminal subtype that have not shown evidence of extraosseous spread. However, if this option is utilized, routine radiographic follow-up is recommended, as the recurrence rate of unicystic ameloblastoma treated with enucleation and curettage has been shown to be unacceptably high. Multicystic ameloblastomas are not amenable to enucleation and curettage, as this treatment results in an unacceptable recurrence rate and should be addressed with an extended surgical resection ( Table 81-1 ).
| Odontogenic Cysts |
|
| Odontogenic Tumors |
|
| Fibro-osseous Lesions |
|
| Other Lesions |
|
Limitations and Contraindications
The enucleation and curettage procedure is limited in the treatment of multicystic lesions for which the treatment of choice might otherwise be the unicystic counterpart. Benign multicystic lesions of the oral and maxillofacial region may have numerous loculations and invaginations that would make access extremely difficult using even an extraoral approach and almost impossible if using an intraoral approach. In addition, the enucleation process may not remove the pathology in its entirety, and physical and chemical curettage may not be able to access or remove all remnants of the lesion. This will invariably lead to persistence of the lesion, particularly a high-recurrence lesion like the KOT or in aggressive benign lesions such as the multicystic ameloblastoma.
The enucleation and curettage approach is contraindicated in solid locally aggressive benign and malignant lesions. Solid benign aggressive lesions such as ameloblastoma would have an extremely high recurrence rate with enucleation and curettage and require resection with at least 1-cm margins in the mandible and partial maxillectomy. Malignant lesions require a more aggressive composite resection, which is not possible with the enucleation and curettage approach.
Technique: Enucleation and Curettage
Step 1:
Radiographic Evaluation
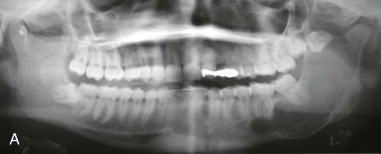
All available radiographic imaging results, such as panoramic radiographs and medical and cone beam CT scans, must be thoroughly assessed. This will help determine the intrabony and soft tissue extent of the lesion and the anatomic structures such as tooth roots and nerves that may be involved ( Figure 81-1, A ).




Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


