Introduction
The purpose of this in-vivo study was to evaluate the effect of a single application of Clinpro XT (3M ESPE, Pymble, New South Wales, Australia), a light-curable fluoride varnish, on enamel demineralization adjacent to orthodontic brackets.
Methods
Thirty-eight patients (152 teeth) whose orthodontic treatment involved extraction of 4 first premolars were recruited. Two premolars each were assigned to the control group (no treatment) and the experimental group (received fluoride varnish application). The study was designed as a nonrandomized split-mouth study in which diagonally opposite quadrants received the same treatment. After the bonding procedures, a sectional T-loop was ligated into each bracket to serve as a site for plaque retention for enhanced demineralization. Clinpro XT was applied on the buccal surfaces adjacent to the brackets on all teeth in the experimental group only. Teeth in both groups were extracted after 15 days (n = 30), 30 days (n = 30), 45 days (n = 30), 90 days (n = 18), and 120 days (n = 18). Buccolingual sections were then evaluated under polarized light microscopy. After we excluded the dropouts, the mean depth of the demineralized enamel lesions was measured in final sample of 126 teeth. The Mann-Whitney test was used for comparison of the groups.
Results
In the control group, the depths of the demineralized enamel lesions increased from 30 to 120 days, whereas in the experimental group no sign of demineralization was noted throughout the observation period except for 3 teeth. Significant differences in the depths of demineralized lesions were found between the study groups.
Conclusions
Clinpro XT light-curable fluoride varnish may be a reasonable alternative in the reduction of enamel demineralization around orthodontic brackets, especially in noncompliant and high-risk patients.
Highlights
- •
Demineralization after application of a light-curable fluoride varnish was assessed.
- •
Demineralization increased in the control group after 30 to 120 days.
- •
Only 3 teeth in the experimental group developed lesions.
- •
Lesion depths differed in the control and experimental group after 30 to 120 days.
- •
A single application of Clinpro XT can prevent demineralization for 120 days.
Enamel demineralization around fixed orthodontic appliances remains the most concerning aspect of fixed appliance therapy. The complex structure of orthodontic brackets makes their periphery an amenable site for the retention of bacterial plaque and hence a potential risk for enamel demineralization. The prevalence of enamel demineralization after fixed orthodontic appliance placement includes up to 50% of patients when no preventive fluoride programs were used.
Fluorides have long played a critical role in the prevention of enamel demineralization during orthodontic treatment. Topical fluorides have been used extensively in the prevention of enamel demineralization around orthodontic brackets. Geiger et al reported a 25% reduction in the number of patients with white spot lesions when they used a home fluoride rinsing program. Stratemann and Shannon found that only 2% of patients on a fluoride regimen developed white spot lesions, whereas 58% of patients without fluoride developed lesions. Nevertheless, the effectiveness of these products is directly related to patient compliance. The difficulty achieving full compliance with a fluoride regimen warrants noncompliance methods with good clinical efficacy.
Fluoride-releasing composites and glass ionomer cements have addressed this problem to some extent, but the bond strength of these materials is lower than conventional composite resin and less than ideal for clinical treatment. Fluoride varnishes are easy to use and do not depend on patient cooperation. The role of conventional fluoride varnishes has been established in both in-vitro and in-vivo studies. However, the longevity and sustainability of these coatings are questionable; therefore, they require repeated applications at specific intervals; this is a cumbersome procedure.
Clinpro XT (3M ESPE, Pymble, New South Wales, Australia) is a highly filled, resin-modified glass ionomer-based light-curable fluoride varnish (LCFV). The varnish layer is claimed to remain intact for more than 5000 brushing strokes and can resist toothbrush abrasion and normal wear for 6 months or longer. The effectiveness of Clinpro XT varnish has been investigated for dentinal hypersensitivity and remineralization, but its role in the reduction of enamel demineralization around orthodontic appliances is not entirely clear. Therefore, the prime objective of this in-vivo study was to evaluate the effect of a single application of Clinpro XT on enamel demineralization adjacent to orthodontic brackets during fixed orthodontic treatment.
Material and methods
This research was designed as a prospective clinical study. Thirty-eight patients aged between 13 and 21 years (mean age, 15.5 years) whose orthodontic treatment involved extraction of 4 first premolars were initially recruited in the orthodontic clinic of Hyderabad Karnataka Education Society, S Nijalingappa Dental College, Gulbarga, Karnataka, India. The sample size was determined using the data for μ1, μ2, and σ from the study of Schmit et al. Assuming a statistical power of 90% and an alpha error of 5%, a minimum of 7 teeth per time period (15, 30, 45, 90, and 120 days) would be necessary in each group. Considering dropouts (we expected 20% to be lost to follow-up), at least 9 teeth per time period in each group were required. To increase the power of the study, a few more were included. The research was approved by the research and ethical committee of our institution.
The inclusion criteria were (1) subjects who consented to all first premolar extractions, (2) all first premolars fully erupted with an intact buccal surface, and (3) no first premolars with clinical evidence of demineralized lesions and fluorosis. We explained the specifics of the study to all subjects, and informed consent was obtained from each subject.
The study was designed so that in each patient the first premolars were allocated to one of the following treatment groups: control group (received no treatment) and experimental group (received fluoride varnish application). We used a nonrandomized split-mouth design in which one quadrant received fluoride varnish application, and the opposite quadrant received no application. The diagonally opposite quadrant received the same treatment. Every alternate patient received the same application pattern in the respective quadrants. Since every patient received varnish application in 2 diagonally opposite quadrants, with no varnish application in the other 2 diagonally opposite quadrants, each patient served his or her own control; hence, the benefit of randomization was achieved through the split-mouth design. This distribution allowed the same environment for all teeth.
After cleaning the teeth with nonfluoridated pumice paste, etching of the enamel surfaces was done with 37% o-phosphoric acid. Standard stainless steel preadjusted edgewise brackets were bonded to the center of teeth with nonfluoridated light-cured composite resin and conventional primer. T-loops of a uniform dimension (0.16 × 0.25-in stainless steel) were ligated to the brackets with elastomeric rings to simulate the clinical situation ( Fig 1 ).

In the experimental group, Clinpro XT was applied on the buccal surfaces surrounding the brackets and then light cured for 1 minute according to the manufacturer’s instructions. All patients were instructed not to brush their teeth for up to 6 hours. Routine oral hygiene instructions were given to each patient to maintain satisfactory oral hygiene, and nonfluoridated toothpaste was advised until the collection of the samples.
At the end of each time period (15, 30, 45, 90, and 120 days), brackets were debonded and the premolars extracted ( Table ). A careful debonding procedure was used to ensure that there were no enamel microfractures around the bracket bases. The roots of all the teeth were cleaned and stored in 0.1% thymol solution. The teeth were embedded in a mold with chemically cured resin to prevent fracturing during thickness reduction. Buccolingual sections were made in the middle third of the crown using a hard tissue microtome (SP1600; Leica, Nussloch, Germany). The thickness of each section was further reduced to 50 to 70 μm by hand grinding. Teeth damaged during the sectioning procedure were discarded. The sections were evaluated under polarized light microscopy (BX51; Olympus, Tokyo, Japan) with xylene as the imbibed medium. Polarized light enables differentiation of enamel lesions in different colors.
| Median ∗ | Minimum | Maximum | Mean ∗ | SD | Z | P value | |
|---|---|---|---|---|---|---|---|
| 15 days | |||||||
| Control (n = 15) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.000 | >0.99 |
| Experimental (n = 15) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 30 days | |||||||
| Control (n = 15) | 40.60 | 35 | 45 | 40.2 | 2.89 | −4.988 | 0.000 † |
| Experimental (n = 15) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | ||
| 45 days | |||||||
| Control (n = 15) | 62.73 | 60 | 70 | 63.7 | 3.39 | −4.987 | 0.000 † |
| Experimental (n = 15) | 0.00 | 0.00 | 0.00 | 00 | 0.00 | ||
| 90 days | |||||||
| Control (n = 9) | 127.70 | 126 | 151 | 130.5 | 7.85 | −3.686 | 0.000 † |
| Experimental (n = 9) | 0.00 | 0.00 | 58 | 10.6 | 21.69 | ||
| 120 days | |||||||
| Control (n = 9) | 217.10 | 160 | 260 | 209.4 | 34.42 | −3.742 | 0.000 † |
| Experimental (n = 9) | 0.00 | 0.00 | 60 | 6.63 | 19.9 | ||
† P <0.001; comparison of lesion depths between control and experimental groups with the Mann-Whitney test; P <0.05 was considered to be significant.
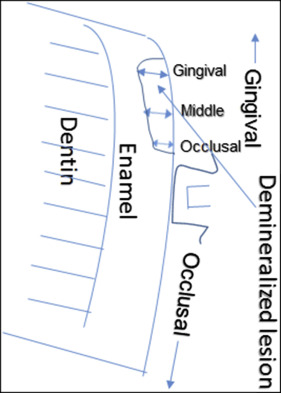
Microphotographs of the gingival half of the buccal surface were taken with fixed magnification of 25 times. In each section, the gingival, middle, and occlusal areas of the demineralized enamel lesions were measured with a scale in the same magnification. The average of these 3 measurements was recorded as the lesion depth for that section ( Fig 2 ). This process was repeated 3 times by 2 oral pathologists in a blinded situation.