Introduction
The literature on tooth dimensions in subjects with Down syndrome (DS) is scarce. To our knowledge, no studies have yet been published in which the morphometry of the teeth in DS subjects has been determined using computed tomography.
Methods
The study group consisted of 40 subjects with DS, aged 10 to 40 years. An age- and sex-matched control group was selected. Cone-beam computed tomography images were retrieved from the archive of the Santiago de Compostela University in Spain. The maxillary central incisors, canines, and first molars were evaluated. The following variables were analyzed: overall tooth length, crown height, root length, mesiodistal diameter, vestibular-palatine diameter, crown-to-root ratio, and cervical circumference.
Results
The teeth of subjects with DS were smaller than those of the controls, although the crown-to-root ratio was maintained. No clear sexual dimorphism was detected, but the root lengths of the incisors were greater in male subjects. Crown height, mesiodistal diameter, and crown-to-root ratio showed progressive reductions with age. There appeared to be a degree of “fluctuating dental asymmetry” with respect to vestibular-palatine diameter and cervical circumference.
Conclusions
Our findings confirm microdontia of the permanent teeth and progressive reductions in tooth sizes with age in persons with DS. These variations might be relevant to orthodontic treatment planning.
Highlights
- •
The maxillary teeth of patients with Down syndrome are smaller than those of the controls.
- •
No clear sexual dimorphism was detected.
- •
Crown dimensions showed a progressive reduction with age.
- •
There appeared to be a degree of “fluctuating dental asymmetry.”
Three-dimensional morphologic evaluation of the teeth is frequently used in anthropology to study differences related to the ethnic origin, age, or sex of subjects. In dentistry, tooth morphometry is used in disciplines as different as periodontology, prosthetics, and orthodontics.
Measurements in these morphologic studies have typically been made directly on jaw casts made from plaster or other stable materials. Although casts accurately represent the dental arches in 3 dimensions, they only allow measurement of crown dimensions. Other 3-dimensional analysis tools developed in recent years, including stereophotogrammetry and laser scanning, allow more complex measurements, such as mesiodistal angulations. Two-dimensional records include digital photographs, panoramic x-rays, and, in particular, periapical x-rays. Cone-beam computed tomography (CBCT) is a new tool for measuring tooth dimensions. This technique can be used to study aspects such as the crown-to-root ratio and dentoalveolar morphometry, and it is more accurate than panoramic x-rays for certain measurements such as root angulation. For crown height and root length, CBCT accuracy is similar to that of periapical x-rays, and its sensitivity in the analysis of root resorption is comparable with that of computed microtomography.
There is a high prevalence of dental abnormalities in patients with Down syndrome (DS), particularly enamel hypoplasia, peg-shaped incisors, and narrow and pointed canines; other abnormalities diagnosed less frequently include transpositions, ankylosis, impaction, root dilacerations, and tooth fusions. It has been reported that 1 of every 4 persons with DS has at least 1 conoid tooth; this abnormality is more common in women and in the maxillary teeth. The permanent teeth are usually small, due mainly to the size of the crown. The prevalence of microdontia is estimated to be between 25% and 55%; although it can affect both deciduous and permanent teeth, microdontia more commonly appears in permanent teeth and can result in spacing. Taurodontia is observed in 33% to 55% of patients, but there is marked variability among studies. Some authors consider this to be the most common dental abnormality in those with DS.
The literature on tooth dimensions in persons with DS is scarce; to our knowledge, no studies have yet been published in which the analysis has been performed using CBCT images. The objective of this study was to use CBCT to determine the crown and root morphologies of the maxillary teeth in subjects with DS.
Material and methods
The study group was formed of 40 white subjects (25 male, 15 female) with DS. The mean age was 18.8 ± 7.3 years (range, 9-43 years). The control group comprised 40 patients without DS matched for age and sex.
All images used in this study were obtained using an i-CAT scanner (Imaging Sciences International, Hatfield, Pa) and belonged to the historical archive of the Radiology Unit of the Faculty of Medicine and Dentistry of the University of Santiago de Compostela in Spain. All scans were performed by 1 technician following the manufacturer’s instructions and standardizing each subject’s position. Only studies in which the complete maxilla was visible were selected. Images were obtained at 120 kVp and 5.0 mA; voxel size was 0.3 mm, with a field of view of 10 to 20 cm and an exposure time of 8.9 seconds. All images were reconstructed with i-CAT Vision software (Imaging Sciences International) and exported using the DICOM format to a MacBook 27 personal computer (Mac OsX 10.6; Apple, Cupertino, Calif). Measurements were made using the open-source OsiriX medical image processing software (Pixmeo, Geneva, Switzerland; www.osirix.viewer.com ).
No specific informed consent was required because all participants or, as appropriate, their legal representatives had signed an informed consent to authorize the use of the images for teaching or research purposes. The study was approved by the institutional review board of the University of Santiago de Compostela.
For the analysis of tooth morphometry, the CBCT images were oriented using multiplanar reconstruction, with a 200% zoom and the modification of the method described by Sherrard et al. First, the sagittal, axial, and coronal planes were adjusted to intersect on the pulp cavity of the target teeth of the study: the maxillary central incisors, the maxillary canines, and the palatal root of the maxillary first molars ( Figs 1-4 ). The axial and coronal planes were then moved on the sagittal plane to intersect at the center of the tooth. In this same sagittal projection, the axial plane was moved until it was at the level of the cementoenamel junction on the buccal and palatal aspects of the tooth ( Figs 1-4 ).
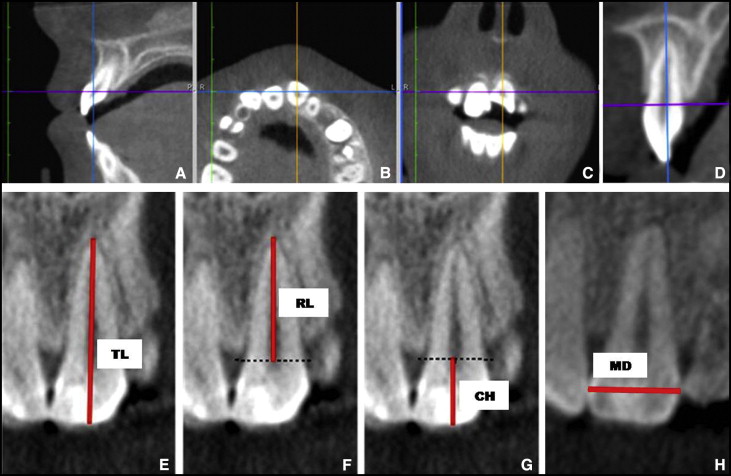
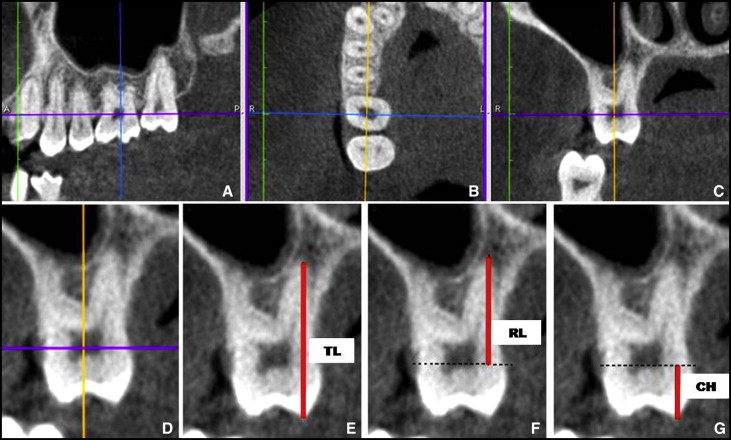
After each target tooth was positioned, overall tooth length, root length, and crown height were measured in the coronal plane. Overall tooth length was calculated as the distance from the incisal edge of the central incisor ( Fig 1 ) or the canine to the apex of the tooth, and in the case of the first molar from the tip of the mesiopalatal cusp to the apex of the palatal root ( Fig 2 ). Root length was measured by drawing a perpendicular line from the line between the buccal and palatal limits of the cementoenamel junction to the apex of the tooth or the palatal root, respectively ( Figs 1 and 2 ). To measure crown height, a perpendicular line was drawn from the line between the buccal and palatal limits of the cementoenamel junction to the incisal edge ( Fig 1 ) or the tip of the mesiopalatal cusp in the case of the first molar ( Fig 2 ). The crown-to-root ratio was defined as the ratio of crown height to root length. Further measurements made in the coronal plane after positioning the tooth were the maximum mesiodistal dimensions of the maxillary central incisors and maxillary canines at the level of the radiographic crown; this was called the mesiodistal diameter ( Fig 1 )
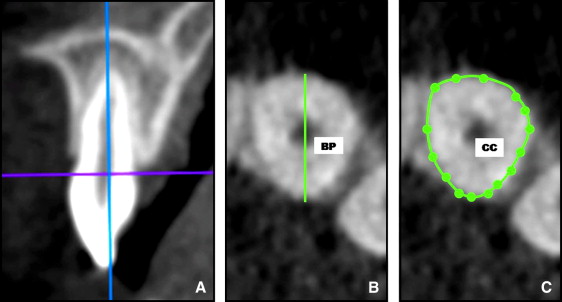
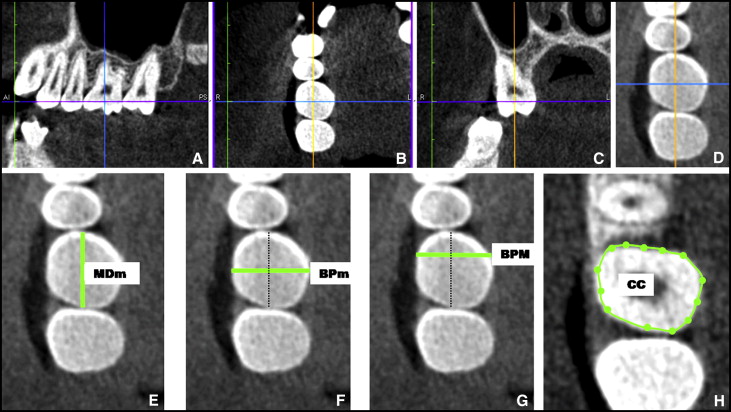
The measurements made in the axial plane after positioning a maxillary central incisor or canine were the buccal-palatal dimension and the cervical circumference. Buccal-palatal dimension was defined as the maximum distance between the buccal and palatal surfaces of the tooth crown along a line perpendicular to the mesiodistal axis of the tooth ( Fig 3 ). Cervical circumference was given by the circumference of the tooth at the level of the cementoenamel junction ( Fig 3 ). The measurements made on the maxillary first molar were the midmesiodistal diameter, midbuccal-palatal diameter, maximum buccal-palatal diameter, and cervical circumference. Midmesiodistal diameter was defined as the distance between the interproximal contact points, midbuccal-palatal diameter as the buccal-palatal distance on a perpendicular line that crossed the midpoint of the mesiodistal axis of the tooth, and maximum buccal-palatal diameter as the maximum diameter on a line perpendicular to the mesiodistal axis of the tooth ( Fig 4 ). Cervical circumference was defined in the same way as for the incisors and the canines ( Fig 4 ).
Statistical analysis
The intraclass correlation coefficient (ICC) was used to determine interobserver and intraobserver reliabilities. To evaluate interobserver reliability, we randomly selected images from 10 participants (5 with DS, 5 controls); after a 2-hour calibration session, 2 trained observers (M.O., M.D.) performed all measurements on the 6 target teeth. To evaluate intraobserver reliability, we randomly selected the images from 10 participants (5 with DS, 5 controls), and 1 trained observer (M.D.) performed all the measurements on the 6 target teeth twice at an interval of 6 weeks.
As a first step in the analysis, the Kruskal-Wallis test was used to detect possible differences in tooth measurements between male and female subjects. Logistic regression was used to assess the possible relationship between tooth measurements and the binary response representing the groups of participants (DS and control). To assess the association of each measurement and the binary response, odds ratio measures and their corresponding 95% confidences intervals were also calculated.
Furthermore, the influence of age on the tooth measurements was studied using additive models. Additive models are extensions of linear regression models, which allow for nonlinear effects of continuous covariates on a response of interest. Specifically, the additive models considered in this study included the effects of age and group (DS and control), and the interaction of age by group. These models take the following form: tooth measurement = β 0 + group + group × f (age) + ε, where f (.) is unspecified smooth functions, producing separate effects of age in each group. Such functions can be estimated with any of the smoothing techniques. In this study, P-splines were used as smoothers.
To determine the dimensional symmetry between the central incisors, between the canines, and between the first molars, additive mixed models were used for each group (DS and controls). Additive mixed models are extensions of linear mixed models, which enable us to include random effects in addition to the usual fixed effects. In this study, the following additive mixed models including the smooth effect of age, the fixed effects of sex and teeth, and the random effects of patient were considered: tooth measurement = β 0 + f (age) + sex + teeth + random (patient) + ε.
All statistical analyses were carried out with the statistical software R (version 2.12.0; R Development Core Team, Vienna, Austria). With this software, the following packages were used: “mgcv” for fitting additive models and additive mixed models, and “nlme” for fitting linear mixed models.
Results
The intraclass correlation coefficients, taking the DS and the control groups together, were between 0.981 and 0.960 for interobserver reliability, and between 0.984 and 0.999 for intraobserver reliability.
Comparison of the morphometric variables of the central incisors, canines, and first molars between the DS and control groups showed that with the exception of crown-to-root ratio, all values were significantly lower in the subjects with DS. These results are shown in Table I .
| Tooth | Dimension | DS/C mean (mm) | Significance | Odds ratio (95% CI) |
|---|---|---|---|---|
| Maxillary right central incisor | Overall tooth length | 18.95/22.70 | P = 0.001 | 2.14 (1.54, 2.98) |
| Crown height | 8.42/9.86 | P = 0.001 | 3.65 (1.95, 6.84) | |
| Root length | 10.53/12.83 | P = 0.001 | 2.58 (1.67, 4.00) | |
| Mesiodistal diameter | 7.88/8.56 | P = 0.001 | 5.61 (2.18, 14.43) | |
| Buccal-palatal diameter | 6.69/7.27 | P = 0.005 | 3.70 (1.72, 7.97) | |
| Crown-to-root ratio | 0.81/0.77 | P = 0.144 | ||
| Cervical circumference | 18.70/20.74 | P = 0.001 | 5.48 (2.42, 12.38) | |
| Maxillary left central incisor | Overall tooth length | 18.89/23.07 | P = 0.001 | 2.45 (1.65, 3.64) |
| Crown height | 8.53/10.13 | P = 0.001 | 4.29 (2.18, 8.42) | |
| Root length | 10.35/12.91 | P = 0.001 | 2.97 (1.83, 4.83) | |
| Mesiodistal diameter | 7.84/8.50 | P = 0.004 | 3.08 (1.43, 6.67) | |
| Buccal-palatal diameter | 6.34/7.07 | P = 0.001 | 16.50 (4.07, 66.82) | |
| Crown-to-root ratio | 0.83/0.78 | P = 0.057 | ||
| Cervical circumference | 18.87/21.04 | P = 0.001 | 8.96 (3.36, 23.89) | |
| Maxillary right canine | Overall tooth length | 18.66/25.22 | P = 0.001 | 4.50 (1.88, 10.75) |
| Crown height | 6.54/9.43 | P = 0.001 | 38.21 (5.02, 290.82) | |
| Root length | 12.11/15.76 | P = 0.001 | 2.85 (1.85, 4.4) | |
| Mesiodistal diameter | 6.73/7.96 | P = 0.001 | 21.16 (5.73, 78.14) | |
| Buccal-palatal diameter | 6.94/8.31 | P = 0.001 | 40.15 (8.33, 193.54) | |
| Crown-to-root ratio | 0.54/0.59 | P = 0.052 | ||
| Cervical circumference | 19.43/22.19 | P = 0.001 | 6.01 (2.69, 13.41) | |
| Maxillary left canine | Overall tooth length | 18.79/31.04 | P = 0.001 | 4.42 (1.92, 10.17) |
| Crown height | 6.82/9.51 | P = 0.001 | 9.93 (3.58, 27.54) | |
| Root length | 11.96/15.69 | P = 0.001 | 4.12 (2.16, 7.87) | |
| Mesiodistal diameter | 6.78/7.87 | P = 0.001 | 18.72 (4.96, 70.63) | |
| Buccal-palatal diameter | 7.04/8.48 | P = 0.001 | 9.81 (3.85, 25) | |
| Crown-to-root ratio | 0.57/0.58 | P = 0.600 | ||
| Cervical circumference | 19.17/22.39 | P = 0.001 | 5.57 (2.64, 11.77) | |
| Maxillary right first molar | Overall tooth length | 18.49/21.10 | P = 0.001 | 2.98 (1.82, 4.89) |
| Crown height | 5.95/7.10 | P = 0.001 | 10.9 (3.96, 30.02) | |
| Root length | 12.47/14.23 | P = 0.001 | 3.42 (1.93, 6.06) | |
| Midmesiodistal diameter | 9.571/0.04 | P = 0.008 | 3.52 (1.35, 9.18) | |
| Midbuccal-palatal diameter | 9.38/10.82 | P = 0.001 | 10.32 (3.54, 30.1) | |
| Maximum buccal-palatal diameter | 9.74/11.51 | P = 0.001 | 18.72 (5.59, 62.65) | |
| Crown-to-root ratio | 0.48/0.49 | P = 0.480 | ||
| Cervical circumference | 29.25/32.82 | P = 0.001 | 3.15 (1.94, 5.14) | |
| Maxillary left first molar | Overall tooth length | 18.73/21.40 | P = 0.001 | 11.05 (3.02, 40.41) |
| Crown height | 6.10/7.14 | P = 0.001 | 16.24 (4.38, 60.14) | |
| Root length | 12.63/14.24 | P = 0.001 | 7.98 (2.87, 22.16) | |
| Midmesiodistal diameter | 9.73/10.35 | P = 0.001 | 3.17 (1.47, 6.82) | |
| Midbuccal-palatal diameter | 9.59/10.64 | P = 0.001 | 6.92 (2.63, 18.2) | |
| Maximum buccal-palatal diameter | 10.01/11.5 | P = 0.001 | 56.23 (9.21, 343.22) | |
| Crown-to-root ratio | 0.48/0.49 | P = 0.530 | ||
| Cervical circumference | 29.57/32.31 | P = 0.001 | 3.05 (1.87, 4.96) |
In the DS group, no significant differences were observed between the sexes in any of the variables analyzed. Nor were significant differences found on comparing the dimensions of the maxillary incisors, canines, and first molars between male and female subjects in the control group.
In the DS group, the additive model demonstrated that numerous morphometric variables of the maxillary central incisors changed significantly with age. Overall tooth length decreased because of reduction in crown height, and there were progressive decreases in mesiodistal diameter and crown-to-root ratio ( Table II ). The progressive decrease of mesiodistal diameter with age was also detected in the canines; in addition, in the maxillary left canine, overall tooth length decreased because of the reduction in crown height ( Table II ). The maxillary right first molar also showed significant decreases in overall tooth length, crown height, and mesiodistal diameter with age. In contrast, none of the variables analyzed on the maxillary left first molar varied significantly with age ( Table II ). In the control group, the morphometric tooth variables were not affected by age.
| Tooth | Variable | Additive model | |
|---|---|---|---|
| Explained variance | Significance DS*f(Age) |
||
| Maxillary right central incisor | Overall tooth length | 48.6% | P = 0.002 |
| Crown height | 46.8% | P = 0.001 | |
| Root length | 47.6% | P = 0.069 | |
| Mesiodistal diameter | 44.1% | P = 0.006 | |
| Buccal-palatal diameter | 22.0% | P = 0.052 | |
| Crown-to-root ratio | 32.0% | P = 0.006 | |
| Cervical circumference | 45.1% | P = 0.035 | |
| Maxillary left central incisor | Overall tooth length | 60.6% | P = 0.001 |
| Crown height | 57.3% | P = 0.001 | |
| Root length | 50.5% | P = 0.140 | |
| Mesiodistal diameter | 26.0% | P = 0.032 | |
| Buccal-palatal diameter | 42.2% | P = 0.007 | |
| Crown-to-root ratio | 40.5% | P = 0.001 | |
| Cervical circumference | 56.0% | P = 0.240 | |
| Maxillary right canine | Overall tooth length | 84.0% | P = 0.011 |
| Crown height | 84.4% | P = 0.016 | |
| Root length | 69.2% | P = 0.160 | |
| Mesiodistal diameter | 64.4% | P = 0.004 | |
| Buccal-palatal diameter | 56.4% | P = 0.662 | |
| Crown-to-root ratio | 20.2% | P = 0.306 | |
| Cervical circumference | 62.5% | P = 0.251 | |
| Maxillary left canine | Overall tooth length | 99.5% | P = 0.020 |
| Crown height | 76.1% | P = 0.001 | |
| Root length | 78.1% | P = 0.063 | |
| Mesiodistal diameter | 64.4% | P = 0.003 | |
| Buccal-palatal diameter | 61.1% | P = 0.940 | |
| Crown-to-root ratio | 35.8% | P = 0.176 | |
| Cervical circumference | 74.2% | P = 0.102 | |
| Maxillary right first molar | Overall tooth length | 43.1% | P = 0.014 |
| Crown height | 46.7% | P = 0.029 | |
| Root length | 38.1% | P = 0.008 | |
| Midmesiodistal diameter | 48.6% | P = 0.001 | |
| Midbuccal-palatal diameter | 57.8% | P = 0.279 | |
| Maximum buccal-palatal diameter | 69.1% | P = 0.424 | |
| Crown-to-root ratio | 12.9% | P = 0.318 | |
| Cervical circumference | 73.0% | P = 0.010 | |
| Maxillary left first molar | Overall tooth length | 53.2% | P = 0.720 |
| Crown height | 37.5% | P = 0.641 | |
| Root length | 35.1% | P = 0.899 | |
| Midmesiodistal diameter | 28.4% | P = 0.339 | |
| Midbuccal-palatal diameter | 35.0% | P = 0.493 | |
| Maximum buccal-palatal diameter | 66.9% | P = 0.277 | |
| Crown-to-root ratio | 4.0% | P = 0.953 | |
| Cervical circumference | 53.5% | P = 0.489 | |
Analysis of the symmetry of the maxillary central incisors showed no significant differences in buccal-palatal diameter between the 2 teeth in subjects with DS, whereas in the control group, differences were present in cervical circumference ( Table III ). Significant differences were found in crown height and crown-to-root ratio of the maxillary canines in the DS group ( Table IV ). Statistically significant differences in maximum buccal-palatal diameter were observed between the maxillary first molars in the DS group, whereas differences were detected in mesiodistal diameter and cervical circumference in the control group ( Table V ).


