Introduction
The aims of this study were to quantitatively evaluate the changes in arch widths and buccolingual inclinations of the posterior teeth after asymmetric rapid maxillary expansion (ARME) and to compare the measurements between the crossbite and the noncrossbite sides with cone-beam computed tomography (CBCT).
Methods
From our clinic archives, we selected the CBCT records of 30 patients with unilateral skeletal crossbite (13 boys, 14.2 ± 1.3 years old; 17 girls, 13.8 ± 1.3 years old) who underwent ARME treatment. A modified acrylic bonded rapid maxillary expansion appliance including an occlusal locking mechanism was used in all patients. CBCT records had been taken before ARME treatment and after a 3-month retention period. Fourteen angular and 80 linear measurements were taken for the maxilla and the mandible. Frontally clipped CBCT images were used for the evaluation. Paired sample and independent sample t tests were used for statistical comparisons.
Results
Comparisons of the before-treatment and after-retention measurements showed that the arch widths and buccolingual inclinations of the posterior teeth increased significantly on the crossbite side of the maxilla and on the noncrossbite side of the mandible ( P <0.05). Comparison of the 2 sides showed statistically significant differences in both the maxilla and the mandible ( P <0.05).
Conclusions
After ARME treatment, the crossbite side of the maxilla and the noncrossbite side of the mandible were more affected than were the opposite sides.
Highlights
- •
The asymmetric rapid maxillary expansion appliance (ARME) effectively treats true unilateral posterior crossbites.
- •
All maxillary and mandibular arch widths increased after treatment with the ARME.
- •
All maxillary and mandibular posterior teeth tipped buccally after treatment with the ARME.
- •
ARME gave anchorage control on the maxillary noncrossbite side and expansion on the crossbite side.
- •
The noncrossbite side of the mandible was more affected than the opposite side after ARME treatment.
Posterior crossbite, a common malocclusion in patients seeking orthodontic treatment, can be either a unilateral or a bilateral malocclusion of the deciduous, mixed, or permanent dentition. The incidence of posterior crossbite ranges from 7% to 23%, with unilateral crossbite being predominant. Unilateral posterior crossbite includes the teeth on 1 side of the arch and can be defined as either a functional posterior crossbite or a true unilateral posterior crossbite. In a functional posterior crossbite, mild bilateral constriction of the maxillary arch that creates occlusal interferences leads to a functional shift of the mandible toward the crossbite side upon closure. In a true unilateral posterior crossbite from intra-arch or jaw asymmetry, a crossbite is seen in both centric relation and centric occlusion without a functional shift of the mandible.
Posterior crossbite is frequently caused by a transverse maxillary skeletal deficiency that may have an underlying congenital, developmental, traumatic, or iatrogenic cause. Therefore, posterior crossbite treatment often aims to achieve maxillary expansion. However, expansion modalities in posterior crossbite treatment differ depending on whether the unilateral posterior crossbite is functional or true and considering the diagnostic findings. Treating a functional posterior crossbite usually involves symmetric expansion of the maxillary arch and elimination of the mandibular functional shift. In a true unilateral posterior crossbite, asymmetric expansion should expand the constricted side of the maxillary arch and avoid overexpanding the unaffected side. Thus far, several asymmetric maxillary expansion devices have been used for correcting true unilateral posterior crossbites, the effects of which were assessed using dental models and lateral and posteroanterior cephalograms.
For decades, orthodontists have largely been bounded by 2-dimensional analyses for researching the effects of maxillary expansion; the advent of cone-beam computed tomography (CBCT) has added the third dimension. CBCT for the maxillofacial region enables multiplanar imaging and provides 3-dimensional (3D) information, allowing for measurement of axial inclinations of the dentition and changes in the transverse dimensions free from distortion, magnification, and superimposition. CBCT imaging provides submillimeter resolution images (isotropic resolution, 0.4-0.125 mm) with relatively short scanning times (10-70 seconds) and a reduced radiation dose (equivalent to that needed for 4-15 panoramic radiographs).
The effects of rapid maxillary expansion (RME) on the dentoskeletal complex have been studied using dental casts, lateral and posteroanterior cephalograms, and CBCT. To the best of our knowledge, no studies conducted thus far have evaluated the effects of asymmetric rapid maxillary expansion (ARME) on the dentoskeletal complex with CBCT. Therefore, the aims of this study were to quantitatively evaluate the changes in arch widths and buccolingual inclinations of posterior teeth after ARME treatment and to compare the measurements between the crossbite and noncrossbite sides using CBCT. The null hypothesis was that there are no statistically significant differences in arch widths and buccolingual inclinations of the posterior teeth between the crossbite and noncrossbite sides after treatment with ARME.
Material and methods
Sample size estimation was based on the standard deviations of a similar study by Kartalian et al, who found a statistically significant increase of 5.42 ± 3.02 mm in external molar widths. Assuming an increase of 25% in this previous finding, with an α error of 0.05 and a power of 80%, we calculated that our sample size should be 30 patients per group.
The CBCT records of 30 patients with unilateral skeletal crossbite (13 boys: mean age, 14.2 ± 1.3 years; range, 12.5-16 years; and 17 girls: mean age, 13.8 ± 1.3 years; range, 12.3-15.4 years) who underwent treatment with ARME were selected from the archives of the Department of Orthodontics of Selcuk University, Konya, Turkey. Ninety-six patients with unilateral posterior crossbites were admitted to our orthodontic department from 2010 to 2013, and 39 of them had unilateral skeletal crossbites. Thirty patients who met the inclusion criteria were selected for this study. All patients were in the permanent dentition and had unilateral posterior crossbites of the nonfunctional type with coincident midlines. In 14 patients, the crossbite was on the left side; in 16, it was on the right side. Any relationship of the unilateral posterior crossbite and the mandibular shift was evaluated clinically. The patients had no craniofacial abnormalities or previous surgical or extraction treatment. The same orthodontist (Z.I.) treated all patients. Ethical approval for this study was obtained from the regional ethical committee on research of Selcuk University.
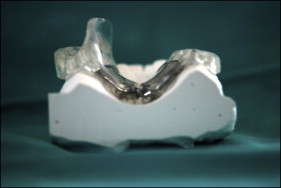
The ARME appliance used was built by adding an occlusal locking mechanism to a modified acrylic bonded RME appliance. The modified acrylic bonded RME appliance was a splint-type tooth and tissue-borne appliance ( Fig 1 ). The acrylic part of the appliance extended over the occlusal and middle thirds of the vestibular surfaces of all teeth. A hyrax screw (Dentaurum, Pforzheim, Germany) was placed in the acrylic plate parallel to the second premolars and as near to the palate as possible. Holes were drilled on the cusps of the maxillary teeth on the ARME appliance to allow escape of the luting cement. On the noncrossbite side, an acrylic extension was formed that extended vertically from the palatal part of the maxillary posterior teeth to the lingual part of the mandibular posterior teeth. The acrylic part of the appliance extended to the middle third of the vestibular surfaces of the mandibular posterior teeth after forming the occlusal tracks of these teeth. The occlusal locking mechanism was formed by covering the lingual and vestibular aspects of the mandibular posterior teeth with acrylic.
The appliance was activated with a quarter turn twice per day in the first week to overcome the resistance of the sutures and once per day after the sutures were mobilized. Expansion was stopped when the holes on the palatal cusps of the maxillary posterior teeth occluded with the buccal cusps of the mandibular posterior teeth (average time, 4-6 weeks). The expander was used for retention for the first 3 months and then replaced with a transpalatal arch.
All CBCT images were obtained with a Kodak unit (model CS 9300; Carestream Health, Rochester, NY) set as follows: exposures were made at 8.0 mA and 70 kV for 6.15 seconds with an axial slice thickness of 0.18 mm. The patients were asked to put their heads in the Frankfort horizontal position for the CBCT scans. The DICOM images were imported, and cross-sectional slices were obtained using Mimics software (version 14.01; Materialise, Leuven, Belgium). To establish the standard orientation of the craniofacial structures, 3-dimensional reference planes were set. The Frankfort horizontal plane was defined as the plane that passed through bilateral porion and right orbitale. The midsagittal plane was defined as the plane perpendicular to the horizontal plane passing through nasion and the midporion point. The frontal plane was constructed from nasion and perpendicular to the horizontal and midsagittal planes. Each 3-dimensional rendered image was then reoriented using the Frankfort horizontal, midsagittal, and horizontal planes. All transverse linear and angular measurements were recorded for each scan before ARME treatment (T1) and after a 3-month retention period (T2). One investigator (M.A.) took all measurements.
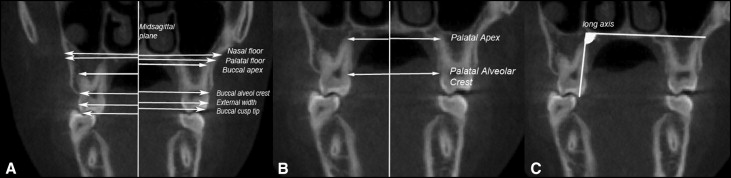
In this study, 40 linear and 6 angular measurements of the maxilla were taken ( Fig 2 ). Kartalian et al described the linear and angular measurements for the maxilla and the maxillary teeth. The nasal floor was assessed relative to the midsagittal plane, parallel to the lower border of the hard palate and tangent to the nasal floor at its most superior level. The palatal floor was also assessed relative to the midsagittal plane, parallel to the lower border of the hard palate and tangent to the hard palate. The external maxillary linear measurements were taken relative to the midsagittal plane at the buccal alveolar crest, the most prominent point of the crown at the buccal aspect, the buccal cusp tip, the apex of the buccal root levels of the maxillary first and second premolars, and the maxillary first molars on the crossbite and noncrossbite sides. The internal maxillary linear measurements were taken relative to the midsagittal plane at the apex of the palatal root and the palatal alveolar crest levels of each included tooth on the crossbite and noncrossbite sides. The angular measurements of maxillary teeth were taken relative to a horizontal reference line parallel to the palatal plane. The angle between the long axis of the maxillary teeth and the reference line was measured for the crossbite and the noncrossbite sides.
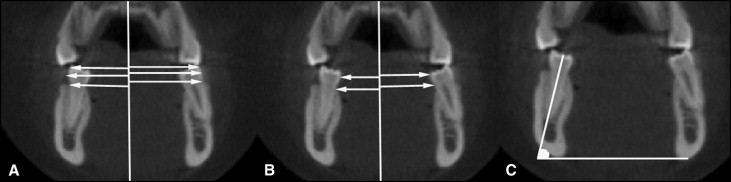
Forty linear and 8 angular measurements were taken of the mandible ( Fig 3 ). Baysal et al described the linear and angular measurements for the mandible and the mandibular teeth. The external mandibular linear measurements were taken relative to the midsagittal plane at the buccal alveolar crest, the most prominent point of the crown at the buccal aspect, the buccal cusp tip levels of the mandibular canines, the mandibular first and second premolars, and the mandibular first molars on the crossbite and noncrossbite sides. The internal mandibular linear measurements were taken relative to the midsagittal plane at the most prominent point of the crown at the lingual aspect and the lingual alveolar crest levels of each included tooth on the crossbite and noncrossbite sides. The angular measurements of the mandibular teeth were taken by considering a horizontal reference line passing through the lower borders of the mandible. The angle between the long axis of the mandibular teeth and the reference line was measured for the crossbite and noncrossbite sides.
Statistical analysis
The Statistical Package for the Social Sciences (version 17.0; SPSS, Chicago, Ill) was used for data analysis, and a P value of <0.05 was considered to be statistically significant. Numeric data are given as means and standard deviations. Twenty CBCT images were randomly selected, and the same investigator (M.A.) repeated the initial measurements of each side 30 days after the first measurements. Intraclass correlation coefficients were performed to assess the reliability of the measurements, as described by Houston, in the same images: the coefficients of reliability for the measurements were greater than 0.918. In addition, a paired t test was used to test the difference between the 2 tracings; no significant difference was found ( P >0.05), confirming the intraobserver reliability of the measurements.
The Shapiro-Wilk test for normality and the Levene test for variance homogeneity were applied to the data. The data at T1 and T2 were found to be normally distributed, and homogeneity of variance was noted among the groups. Therefore, the statistical evaluations of these data were performed using parametric tests. Statistically significant differences between the 2 sides were determined with the independent t test. The paired t test was used to determine the differences in mean changes in each side.
Results
The descriptive statistics and intragroup comparisons of the crossbite and noncrossbite sides are shown in Table I for the maxillary linear measurements. All maxillary linear and angular measurements increased after treatment with ARME. T1 to T2 comparisons showed that these increases were statistically significant on the crossbite side of the maxilla ( P <0.05). Comparison of changes in the maxillary linear measurements between the 2 sides showed statistically significant differences ( Table II ; P <0.05). The descriptive statistics and intragroup comparisons of the crossbite and noncrossbite sides are shown in Table III for the maxillary angular measurements. Comparisons of the changes in maxillary angular measurements between the 2 sides showed statistically significant differences ( Table IV ; P <0.001).
| n | T1 | T2 | Significance | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Maxillary linear measurements | ||||||
| Nasal floor-Y | ||||||
| Crossbite side | 30 | 31.24 | 1.78 | 33.17 | 1.69 | ∗ |
| Noncrossbite side | 30 | 32.64 | 1.81 | 32.91 | 1.83 | NS |
| Palatal floor-Y | ||||||
| Crossbite side | 30 | 28.62 | 1.57 | 31.47 | 1.72 | † |
| Noncrossbite side | 30 | 30.28 | 1.75 | 30.89 | 2.04 | NS |
| External | ||||||
| Apex | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 14.76 | 0.93 | 18.25 | 1.19 | † |
| Second premolar-Y | 30 | 17.08 | 1.03 | 20.01 | 1.27 | ∗ |
| First molar-Y | 30 | 18.27 | 1.41 | 20.62 | 1.52 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 18.78 | 1.45 | 19.21 | 1.59 | NS |
| Second premolar-Y | 30 | 19.62 | 1.53 | 20.04 | 1.63 | NS |
| First molar-Y | 30 | 19.92 | 1.50 | 20.45 | 1.74 | NS |
| Alveolar crest | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 19.03 | 1.62 | 22.67 | 1.89 | † |
| Second premolar-Y | 30 | 21.32 | 2.01 | 24.28 | 1.93 | † |
| First molar-Y | 30 | 25.67 | 1.79 | 28.46 | 1.94 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 21.37 | 1.68 | 22.05 | 1.54 | NS |
| Second premolar-Y | 30 | 22.79 | 1.83 | 23.19 | 2.08 | NS |
| First molar-Y | 30 | 27.19 | 1.80 | 27.88 | 2.17 | NS |
| Buccal | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 18.92 | 1.75 | 22.19 | 1.93 | † |
| Second premolar-Y | 30 | 21.27 | 2.09 | 24.38 | 2.31 | † |
| First molar-Y | 30 | 26.02 | 1.99 | 28.95 | 2.17 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 21.49 | 2.14 | 22.26 | 2.10 | NS |
| Second premolar-Y | 30 | 22.57 | 2.13 | 23.21 | 2.06 | NS |
| First molar-Y | 30 | 27.03 | 1.88 | 27.92 | 2.08 | NS |
| Occlusal | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 16.14 | 1.45 | 19.72 | 1.67 | † |
| Second premolar-Y | 30 | 19.23 | 1.57 | 22.09 | 1.64 | † |
| First molar-Y | 30 | 23.87 | 2.07 | 26.02 | 2.13 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 18.11 | 1.94 | 18.92 | 2.27 | NS |
| Second premolar-Y | 30 | 20.68 | 2.04 | 21.20 | 1.99 | NS |
| First molar-Y | 30 | 24.92 | 2.27 | 25.52 | 2.09 | NS |
| Internal | ||||||
| Palatal apex | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 11.23 | 0.73 | 14.86 | 0.89 | † |
| Second premolar-Y | 30 | 14.02 | 0.83 | 17.17 | 0.90 | † |
| First molar-Y | 30 | 14.62 | 0.92 | 17.21 | 0.88 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 13.84 | 0.91 | 14.32 | 0.97 | NS |
| Second premolar-Y | 30 | 16.34 | 1.04 | 16.85 | 0.91 | NS |
| First molar-Y | 30 | 16.68 | 1.12 | 17.02 | 0.99 | NS |
| Palatal alveolar crest | ||||||
| Crossbite side | ||||||
| First premolar-Y | 30 | 12.04 | 0.81 | 14.97 | 1.03 | † |
| Second premolar-Y | 30 | 14.47 | 1.08 | 17.62 | 1.27 | † |
| First molar-Y | 30 | 15.79 | 1.17 | 18.08 | 1.31 | ∗ |
| Noncrossbite side | ||||||
| First premolar-Y | 30 | 14.11 | 0.97 | 14.62 | 1.20 | NS |
| Second premolar-Y | 30 | 16.84 | 1.13 | 17.32 | 1.22 | NS |
| First molar-Y | 30 | 17.65 | 1.25 | 18.12 | 1.32 | NS |
| Mandibular linear measurements | ||||||
| External | ||||||
| Occlusal | ||||||
| Crossbite side | ||||||
| Canine-Y | 30 | 13.21 | 1.13 | 13.45 | 1.03 | NS |
| First premolar-Y | 30 | 18.84 | 1.25 | 18.97 | 1.17 | NS |
| Second premolar-Y | 30 | 20.54 | 1.35 | 20.82 | 1.21 | NS |
| First molar-Y | 30 | 26.91 | 1.31 | 28.03 | 1.33 | ∗ |
| Noncrossbite side | ||||||
| Canine-Y | 30 | 12.10 | 1.12 | 13.72 | 1.28 | ∗ |
| First premolar-Y | 30 | 16.92 | 1.19 | 18.74 | 1.31 | ∗ |
| Second premolar-Y | 30 | 19.05 | 1.22 | 21.13 | 1.28 | † |
| First molar-Y | 30 | 25.82 | 1.53 | 28.02 | 1.37 | † |
| Buccal | ||||||
| Crossbite side | ||||||
| Canine-Y | 30 | 17.82 | 0.98 | 18.32 | 1.05 | NS |
| First premolar-Y | 30 | 19.82 | 1.13 | 20.35 | 1.20 | NS |
| Second premolar-Y | 30 | 24.22 | 1.42 | 25.06 | 1.33 | NS |
| First molar-Y | 30 | 28.23 | 1.72 | 29.41 | 1.63 | ∗ |
| Noncrossbite side | ||||||
| Canine-Y | 30 | 16.37 | 1.05 | 18.05 | 1.17 | ∗ |
| First premolar-Y | 30 | 19.04 | 1.23 | 21.02 | 1.27 | ∗ |
| Second premolar-Y | 30 | 24.16 | 1.31 | 26.04 | 1.25 | ∗ |
| First molar-Y | 30 | 27.89 | 1.52 | 29.75 | 1.64 | ∗ |
| Alveolar crest | ||||||
| Crossbite side | ||||||
| Canine-Y | 30 | 16.42 | 1.41 | 17.03 | 1.36 | NS |
| First premolar-Y | 30 | 20.35 | 1.51 | 21.03 | 1.44 | NS |
| Second premolar-Y | 30 | 24.68 | 1.73 | 26.19 | 1.67 | ∗ |
| First molar-Y | 30 | 28.13 | 1.49 | 29.78 | 1.66 | ∗ |
| Noncrossbite side | ||||||
| Canine-Y | 30 | 16.68 | 1.26 | 17.62 | 1.34 | NS |
| First premolar-Y | 30 | 19.74 | 1.55 | 21.92 | 1.61 | ∗ |
| Second premolar-Y | 30 | 25.72 | 1.73 | 27.45 | 1.88 | ∗ |
| First molar-Y | 30 | 28.37 | 1.64 | 31.05 | 1.81 | † |
| Internal | ||||||
| Lingual | ||||||
| Crossbite side | ||||||
| Canine-Y | 30 | 12.04 | 0.92 | 12.42 | 1.07 | NS |
| First premolar-Y | 30 | 14.73 | 1.08 | 15.27 | 1.14 | NS |
| Second premolar-Y | 30 | 16.14 | 1.20 | 16.82 | 1.15 | NS |
| First molar-Y | 30 | 18.32 | 1.35 | 19.73 | 1.29 | ∗ |
| Noncrossbite side | ||||||
| Canine-Y | 30 | 11.45 | 0.84 | 12.62 | 0.91 | ∗ |
| First premolar-Y | 30 | 13.83 | 0.95 | 15.22 | 1.04 | ∗ |
| Second premolar-Y | 30 | 15.56 | 1.14 | 17.24 | 1.22 | ∗ |
| First molar-Y | 30 | 17.63 | 1.31 | 19.91 | 1.28 | † |
| Alveolar crest | ||||||
| Crossbite side | ||||||
| Canine-Y | 30 | 12.01 | 1.03 | 12.39 | 0.89 | NS |
| First premolar-Y | 30 | 15.12 | 1.11 | 15.53 | 0.93 | NS |
| Second premolar-Y | 30 | 17.34 | 1.26 | 18.63 | 1.47 | ∗ |
| First molar-Y | 30 | 19.32 | 1.36 | 20.43 | 1.52 | ∗ |
| Noncrossbite side | ||||||
| Canine-Y | 30 | 11.34 | 0.79 | 13.03 | 0.93 | ∗ |
| First premolar-Y | 30 | 14.45 | 1.06 | 16.89 | 1.18 | ∗ |
| Second premolar-Y | 30 | 16.67 | 1.19 | 19.34 | 1.37 | † |
| First molar-Y | 30 | 18.72 | 1.54 | 22.03 | 1.62 | † |
| n | Crossbite side | Noncrossbite side | Significance | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Maxillary linear measurements | ||||||
| Nasal floor | 30 | 1.93 | 0.93 | 0.27 | 0.29 | † |
| Palatal floor | 30 | 2.85 | 0.87 | 0.61 | 0.54 | ‡ |
| External | ||||||
| Apex | ||||||
| First premolar-Y | 30 | 3.49 | 1.13 | 0.43 | 0.39 | ‡ |
| Second premolar-Y | 30 | 2.93 | 0.89 | 0.42 | 0.32 | ‡ |
| First molar-Y | 30 | 2.35 | 0.94 | 0.53 | 0.37 | † |
| Alveolar crest | ||||||
| First premolar-Y | 30 | 3.64 | 1.21 | 0.68 | 0.48 | ‡ |
| Second premolar-Y | 30 | 2.96 | 1.17 | 0.40 | 0.43 | ‡ |
| First molar-Y | 30 | 2.79 | 1.05 | 0.69 | 0.31 | ‡ |
| Buccal | ||||||
| First premolar-Y | 30 | 3.27 | 1.24 | 0.77 | 0.53 | ‡ |
| Second premolar-Y | 30 | 3.11 | 1.02 | 0.64 | 0.41 | ‡ |
| First molar-Y | 30 | 2.93 | 0.93 | 0.89 | 0.56 | † |
| Occlusal | ||||||
| First premolar-Y | 30 | 3.58 | 0.87 | 0.81 | 0.43 | ‡ |
| Second premolar-Y | 30 | 2.86 | 0.94 | 0.52 | 0.31 | † |
| First molar-Y | 30 | 2.15 | 0.79 | 0.60 | 0.48 | ∗ |
| Internal | ||||||
| Palatal apex | ||||||
| First premolar-Y | 30 | 3.63 | 1.19 | 0.48 | 0.32 | ‡ |
| Second premolar-Y | 30 | 3.15 | 1.08 | 0.51 | 0.46 | ‡ |
| First molar-Y | 30 | 2.59 | 1.02 | 0.34 | 0.32 | ‡ |
| Palatal alveolar crest | ||||||
| First premolar-Y | 30 | 2.93 | 0.93 | 0.51 | 0.37 | ‡ |
| Second premolar-Y | 30 | 3.15 | 0.98 | 0.48 | 0.41 | ‡ |
| First molar-Y | 30 | 2.29 | 0.84 | 0.47 | 0.29 | † |
| Mandibular linear measurements | ||||||
| External | ||||||
| Occlusal | ||||||
| Canine-Y | 30 | 0.24 | 0.54 | 1.62 | 0.62 | † |
| First premolar-Y | 30 | 0.13 | 0.48 | 1.82 | 0.73 | † |
| Second premolar-Y | 30 | 0.28 | 0.38 | 2.08 | 0.70 | † |
| First molar-Y | 30 | 1.12 | 0.92 | 2.20 | 0.73 | ∗ |
| Buccal | ||||||
| Canine-Y | 30 | 0.50 | 0.39 | 1.68 | 0.53 | ∗ |
| First premolar-Y | 30 | 0.53 | 0.42 | 1.98 | 0.78 | † |
| Second premolar-Y | 30 | 0.84 | 0.67 | 1.88 | 0.88 | ∗ |
| First molar-Y | 30 | 1.18 | 1.02 | 1.86 | 0.94 | ∗ |
| Alveolar crest | ||||||
| Canine-Y | 30 | 0.61 | 0.74 | 0.94 | 0.77 | NS |
| First premolar-Y | 30 | 0.68 | 0.59 | 2.18 | 0.69 | † |
| Second premolar-Y | 30 | 1.51 | 1.07 | 1.73 | 1.09 | NS |
| First molar-Y | 30 | 1.65 | 1.12 | 2.68 | 0.97 | ∗ |
| Internal | ||||||
| Lingual | ||||||
| Canine-Y | 30 | 0.38 | 0.62 | 1.17 | 0.88 | ∗ |
| First premolar-Y | 30 | 0.54 | 0.58 | 1.39 | 0.67 | ∗ |
| Second premolar-Y | 30 | 0.68 | 0.61 | 1.68 | 0.78 | ∗ |
| First molar-Y | 30 | 1.41 | 0.99 | 2.28 | 0.84 | NS |
| Alveolar crest | ||||||
| Canine-Y | 30 | 0.38 | 0.62 | 1.69 | 0.82 | ∗ |
| First premolar-Y | 30 | 0.41 | 0.32 | 2.44 | 0.59 | † |
| Second premolar-Y | 30 | 1.29 | 0.51 | 2.67 | 0.79 | ∗ |
| First molar-Y | 30 | 1.11 | 0.78 | 3.31 | 0.96 | † |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


