Ectopic eruption of maxillary canines can be associated with root resorption of adjacent teeth. This case report describes and discusses an interesting case of a 15-year-old girl with a Class III malocclusion and an impacted maxillary canine. Because of the unfavorable position of the ectopic canine and the severe root resorption of the maxillary left central and lateral incisors, the treatment options included extraction of the maxillary permanent canines. The mandibular first premolars were extracted to compensate for the Class III malocclusion. A panoramic radiograph taken earlier in the mixed dentition already indicated a possible eruption disturbance of the maxillary left permanent canine. The importance of early diagnosis of maxillary canine ectopic eruption is highlighted in this case report. The early identification of radiographic signs of an ectopic pathway of eruption should be followed by deciduous canine extraction to prevent canine retention and maxillary incisor root resorption.
Maxillary permanent canines show the highest frequency of impaction, excluding the third molars. According to previous reports, the prevalence of maxillary canine impaction ranges from 0.9% to 2.5%. Although this might seem to be a relatively small prevalence, it is speculated that, in clinical orthodontic practice, the frequency might be higher.
The diagnosis and assessment of the extent of maxillary incisor resorption are fundamentally important for the prevention of impaction and the reduction of subsequent complications of canine eruption. Panoramic radiographs can provide worthwhile information regarding the presence and general location of maxillary canine ectopic eruption in the late mixed dentition. In approximately 80% of patients with impacted canines, the cusp tips overlap the lateral incisor roots during the mixed dentition, as observed in panoramic radiographs. Ericson and Kurol reported that extraction of the maxillary deciduous canines has a favorable effect on maxillary canine ectopic eruption in most patients (78%), if extraction treatment is performed in time, between 10 and 13 years of age.
Root resorption of the maxillary permanent incisors related to maxillary canine ectopic eruption is probably caused by inherent pressure from migration of the displaced erupting canine combined with physical contact between the root of the incisor and the prominence of the canine crown. Associated root resorption of maxillary permanent incisors occurs in 48% of children with maxillary canine ectopic eruption between 9 and 15 years of age, and it is often a serious complication, prolonging orthodontic treatment in many patients. Early diagnosis and intervention could avoid these unfavorable effects. Therefore, the aim of this case report of a patient with severe root resorption of the maxillary incisors related to a palatally displaced canine is to highlight the importance of early diagnosis of maxillary canine ectopic eruption.
Diagnosis and etiology
A 15-year-old girl in the permanent dentition sought orthodontic treatment because of dental crowding in the first author’s private office. The patient was unhappy about the appearance of her smile ( Fig 1 ). At the first appointment, her parents reported that she had already had previous orthodontic treatment with maxillary expansion and facial mask therapy at 8 years of age.

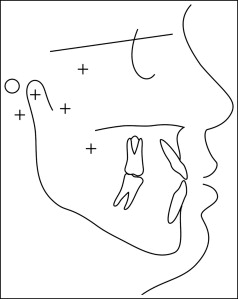
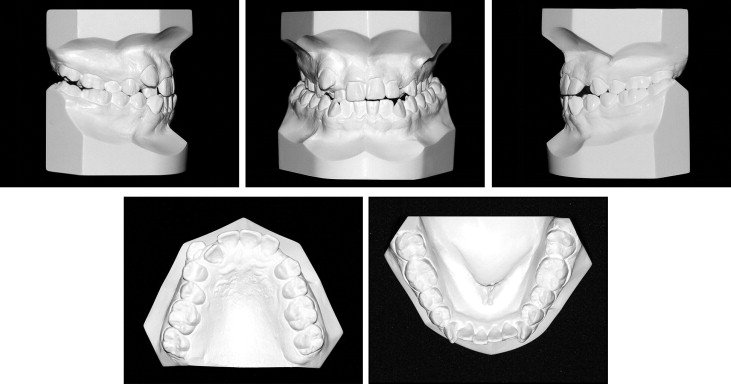
The facial analysis showed a mild Class III skeletal relationship ( Fig 2 ). The intraoral examination revealed a mild Class III molar occlusion with an anterior edge-to-edge relationship, bilateral posterior crossbite, mild mandibular and severe maxillary dental crowding, and an unerupted maxillary left canine. The maxillary right canine was labially displaced ( Fig 3 ). The patient’s oral hygiene was excellent.
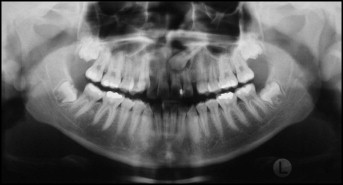
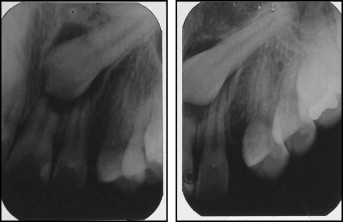
The panoramic radiographic examination confirmed the impaction of the maxillary left canine, which had complete root formation ( Fig 4 ). Periapical radiographs showed severe resorption of the maxillary incisor roots, especially the central incisor, and 2 periapical radiographs taken with Clark’s technique confirmed the palatal displacement of the impacted tooth ( Fig 5 ).
The patient had been previously treated with maxillary expansion and facial mask therapy in the mixed dentition to correct the Class III malocclusion. The panoramic radiograph of the mixed dentition showed signs of ectopic eruption of the maxillary left permanent canine according to the study of Lindauer et al ( Fig 6 ).

Treatment alternatives
One treatment option consisted of maxillary expansion, extraction of the 4 first premolars, surgical exposure, and traction of the maxillary left canine.
The second treatment option included maxillary expansion, and extractions of the mandibular first premolars, and the maxillary right first premolar and left canine.
The third treatment option included maxillary expansion, extractions of the mandibular first premolars and the maxillary right and left canines. The first premolars would replace the canines. This was the selected alternative because of the poor prognosis for canine traction and to obtain symmetry of the anterior section of the maxillary arch.
Treatment progress
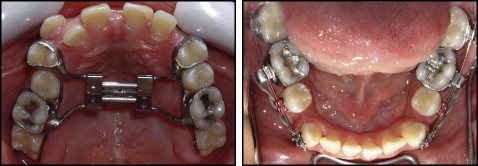
The maxillary arch was expanded with a hyrax expander. Four months after the expansion, the expander was removed, and the mandibular first premolars and the maxillary canines were extracted. Preadjusted 0.022 × 0.025-in fixed appliances were used. Sectional mechanics was used to retract the mandibular canines to maintain the incisor sagittal position ( Fig 7 ). A lip bumper was installed to reinforce anchorage in the mandibular arch. After initial mandibular canine retraction, the incisors were bonded, and leveling and alignment with nickel-titanium archwires (0.012, 0.014, and 0.016 in), followed by stainless steel archwires (0.018, 0.020, and 0.019 × 0.025 in) in both arches, were initiated.
Anterior retraction in the mandibular arch was performed with rectangular stainless steel archwires (0.019 × 0.025 in) and Class III elastics ( Fig 8 ). The Class III elastics also produced mesial drift of the maxillary posterior teeth to close the additional extraction spaces without moving the maxillary incisors, which had short roots. Conventional orthodontic finishing procedures were then undertaken. The total treatment time was 32 months. Retention consisted of a circumferential retainer in the maxillary arch and a bonded canine-to-canine retainer in the mandibular arch.



