The shape and size of tooth roots are genetically and phylogenetically predetermined. Clinical defects in root formation can manifest in the form of shortened roots caused by either root agenesis or root resorption. We report on a patient who came at age 7 years for space management. In the 2-year period after the initial visit, maxillary arch expansion was performed, followed by serial extractions of all 4 first premolars. A radiograph taken about 18 months after the serial extraction showed that although the crowns of all 4 second premolars had erupted fully into the arch, the roots were only about half of their normal length. With a family history of 1 sibling with a missing second premolar and the symmetrical distribution and pattern of the teeth in the 4 dental quadrants, we speculated that the arrested root development was due most likely to a genetic predisposition. Arrested root development is difficult to predict, but a potential warning sign is a family history of malformed or missing teeth. Proper, adequate, and accurate records continue to remain critical for both medical and legal purposes in the treatment of patients with potential problems in root agenesis.
The shape and size of tooth roots are genetically predetermined and phylogenetically conserved. Developmentally, once the crown of a tooth is formed, root genesis starts, and the tooth erupts along a path toward the oral cavity. In the clinical situation, there have been reports of defects in root formation, frequently in the form of roots that are shorter than normal. Shortened roots could be due to either failure of growth or resorption of roots that are already formed. Factors contributing to arrested root development include chemotherapy, radiation therapy, trauma, local factors (eg, infection or hereditary anomalies such as dentin dysplasia type 1 ), and illness (eg, idiopathic hypothyroidism). Unlike arrested root development, root resorption has clearly been shown to be a possible adverse effect of orthodontic tooth movement. However, the exact etiology of root resorption is still unclear, and individual biologic variability, genetic predisposition, and the effect of mechanical factors have been implicated.
In this report, we describe a patient in whom aberrant root development of all 4 second premolars was observed during 2-phase orthodontic treatment, with a pattern of distribution and type that has not been described previously. Radiographic and clinical records gathered over a 7-year period offer an interesting study of the possible causes of the shortened roots and the connection to the orthodontic treatment that was rendered.
Case report
Our patient (age, 7 years 9 months; date of birth, December 22, 1995) came to the office on March 27, 2003, after a referral by a general dentist for monitoring of possible dental crowding in both arches. The patient was a healthy child with no medical problems. An older sister was also being treated in the same orthodontic office for minor crowding and a congenitally missing mandibular left second premolar. Records taken at this appointment showed a mixed dentition stage, with the first permanent molars, the mandibular incisors, and the maxillary left central incisor present intraorally, and the maxillary right central incisor just starting to erupt into the oral cavity (both dental arches in Fig 1 , A ). The panoramic radiograph showed no obvious abnormalities, with a dental age of approximately 7 years 9 months (staged according to standards ) ( Fig 2 , A ). The crowns of the first premolars were almost fully formed; those of the second premolars and the second molars were about two thirds formed, and the roots of the mandibular incisors were almost completely formed, whereas the maxillary incisors were about half formed. The maxillary canines were located relatively high in the bone ( Fig 2 , C ). About 7 months after the initial records were taken (October 2003), the maxillary lateral incisors had erupted fully, and palatal expansion was initiated to address the slight maxillary constriction and the lack of dental arch space. A hyrax expander supported on banded first molars with lateral extensions to the maxillary first deciduous molars was cemented (bands visible in Fig 2 , B ). The expander was activated by 20 turns (5 mm) for 3 weeks to increase the intermolar distance from the central fossae of the maxillary left and right first molars, for a total of 48 mm. The expander was then left in place passively for 3 months before it was removed. Bands were then cemented on the maxillary first molars, and orthodontic brackets were bonded on the maxillary central and lateral incisors to align the anterior segment. Two archwires (round 0.018-in stainless steel, followed 6 months later with a 0.019 × 0.025-in beta-titanium alloy wire) were used to orthodontically align the anterior teeth. After 12 months of treatment, the brackets and the bands were removed (July 6, 2005; Figs 1 , B , and 2 , C ). At this stage, the maxillary and mandibular incisors were well aligned. However, a severe space discrepancy was obvious with minimal spaces for the unerupted maxillary and mandibular canines ( Fig 1 , B ). Furthermore, the maxillary canines were angulated mesially in the panoramic film ( arrowheads in Fig 2 , C ). Because of the severe space discrepancy in both arches, phase 2 treatment began with serial extractions. The roots of the first premolars were slightly more than half formed, whereas the roots of the second premolars looked about half formed ( Fig 2 , C ). The 2 mandibular first deciduous molars were extracted, followed by the removal of all 4 first premolars by an oral surgeon in June 2005, about 3 months after the brackets and bands were removed for phase 1 treatment. Removal of the 6 teeth (2 mandibular first deciduous molars and all 4 first premolars) was performed at the same time at the parent’s request.
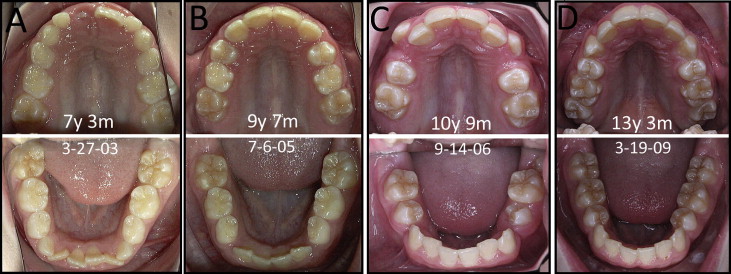
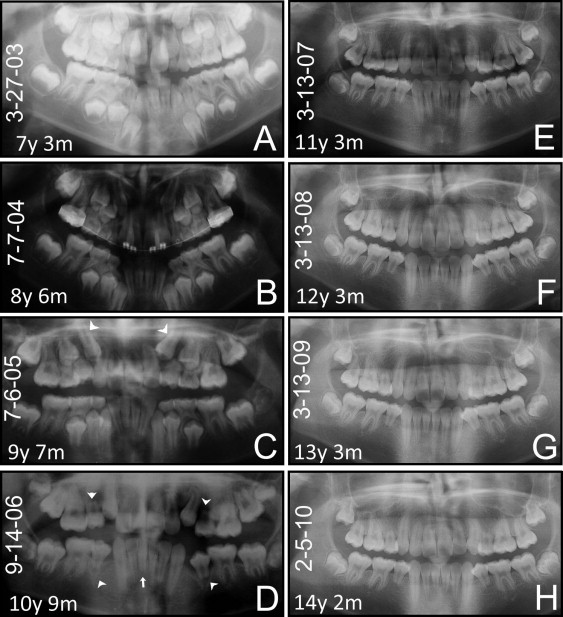
Subsequent follow-up of the patient about a year and half later showed that the roots of the 4 second premolars had not developed ( arrowheads in Fig 2 , D ). The parents were alerted to this unexpected observation. No subsequent orthodontic treatment was rendered, and the patient was followed yearly with no significant changes or worsening of the root formation ( Fig 2 , E-H ).
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


