Introduction
It is unknown whether or not intraoral vibrations affect stick-slip behavior at orthodontic bracket-archwire interfaces. In this study, we evaluated bracket-archwire stick-slip behavior as a function of ligation method and archwire vibration.
Methods
In-vivo archwire vibrations were measured to obtain frequencies and amplitudes for ex-vivo testing. A piezoresistive accelerometer ligated to the maxillary right canines of 6 subjects transduced the intraoral vibrations. All subjects gave informed consent to participate. Amplitude and frequency of the vibrations were quantified and used in a bench-top friction testing apparatus. Active and passive ligation methods were compared for 9 vibration scenarios. The amount of time to move the bracket along a stainless steel wire was recorded in 90 trials. Analysis of variance and post-hoc tests were used for statistical analyses of the data.
Results
During carrot biting, orthodontic wire vibrations had a mean frequency of 98 Hz and a peak-to-peak mean amplitude of 151 mV. The bench-top stick-slip measurement trials containing medium (150 mV) and high (190 mV) amplitude vibrations had significantly less friction (ln, s), 4.81 ± 2.08 and 4.67 ± 2.00, respectively, than those subjected to low (110 mV) amplitudes, 5.80 ± 1.39 ( P = 0.04). There were no significant differences between passive and active ligation methods.
Conclusions
Amplitudes of archwire vibrations affect stick-slip behavior at the bracket-archwire interfaces.
The ability to move a tooth via orthodontic sliding mechanics is, in part, inversely related to the frictional resistance at the bracket-archwire interfaces. Hence, much effort has been applied to decrease the frictional resistance associated with orthodontic appliances. The frictional resistance and subsequent stick-slip behavior at the interfaces between bracket and archwire, as the attached tooth moves by tipping and uprighting, are dictated by the magnitudes of forces normal to the surfaces involved. These normal forces are due to ligation and tipping moments.
Which bracket design provides the least friction is a question that has been explored, by comparing frictional resistances at the bracket-archwire interfaces for various self-ligating brackets, as well as self-ligating vs conventional brackets and ligation methods. However, previous investigations have mainly used steady-state models. Frequently, steady-state experimental setups have drawn a straight archwire through the bracket slot at various speeds and loads by using a universal testing machine. Some of these studies have included an artificial salivary medium, but the role of this artificial saliva on frictional resistance remains inconclusive because of conflicting outcomes. Other studies have attempted to simulate the bracket-archwire contact angle as the tooth attached to the bracket tips during initial movement in vivo. These in-vitro studies have shown that, as bracket slot angulations relative to the archwire increase, so do the frictional resistances at the bracket-archwire interfaces. Although varying research designs have been used, most in-vitro studies have agreed that frictional forces are lower in passive self-ligating compared with active self-ligating brackets, with conventional brackets having the highest frictional resistance. Whereas it is evident that incorporating a clinically relevant tipping moment in vitro better simulates the biomechanical phenomenon of tooth movement during sliding mechanics, further studies are needed to analyze how various bracket designs are affected by the dynamic oral environment.
As early as 1970, the effect of oral forces from mastication in reducing bracket-archwire friction was recognized. Despite this, only a few in-vitro studies have incorporated vibrations at bracket-archwire interfaces to simulate the effects of mastication. Although these studies used arbitrary amounts of vibration, they demonstrated that steady-state models overestimate the impact of friction. For example, Liew placed oscillating forces of 25 to 400 cN at 90 Hz on an archwire as it was drawn through a bracket. This in turn reduced sliding resistance by 60% and 85% with 25 and 100 cN of wire displacement force, respectively. Another study used finger perturbations in 3 planes of space to simulate vibration of the archwire. A mean force of 87.2 cN was used, resulting in kinetic frictional resistance reducing to zero in 95.8% of the experiments. One other published study used a clinically relevant frequency of 81 cycles per minute based on reported values for normal chewing but chose amplitudes of 0, 0.25, 0.5, and 1.0 mm of wire displacement and showed a linear relationship between displacement and friction. To date, no studies in the literature have applied clinically measured frequencies and amplitudes of vibration to ex-vivo friction tests for results that are potentially more pertinent to patient treatment scenarios.
Therefore, the purposes of this study were to obtain in-vivo measurements of vibrational frequencies and amplitudes associated with oral disturbances on orthodontic appliances and then replicate these ex vivo to evaluate the stick-slip behavior at bracket-archwire interfaces by using clinically relevant tipping moments during passive and active bracket ligation. In addition, predictive statistical modeling was applied to the ex-vivo data to explore a broader range of frequencies and amplitudes of vibration and compare potential effects between the 2 types of bracket ligation.
Material and methods
To estimate clinically relevant archwire vibrational characteristics, 6 volunteers participated in the in-vivo component of this study. The protocol was approved by the institutional review board of the University of Missouri-Kansas City, and informed consent was obtained from all participants. The subjects were at least 18 years of age, had maxillary right canines, and were undergoing orthodontic treatment with fixed appliances on their maxillary and mandibular anterior and posterior teeth.
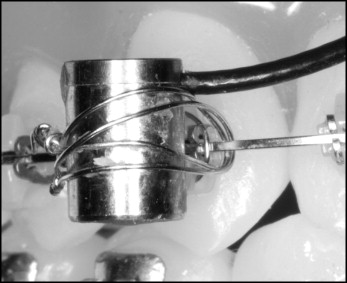
Each subject attended 2 sessions, approximately 2 weeks apart. During each visit, a single-axis piezoresistive accelerometer (model 4374; Bruel & Kjaer, Norcross, Ga) was attached to the maxillary right canine bracket in the occlusogingival direction ( Fig 1 ) with a 0.010-in-diameter stainless steel ligature wire. The sensitivity of the accelerometer was expressed in terms of charge per unit of acceleration and had a value of 0.26 mV/gravity. The range of measureable frequencies was 1 to 26,000 Hz.
The subjects were instructed to incise a raw carrot sample with a 10 × 10 mm cross-section and a 30-mm length oriented parallel to the occlusal plane between the maxillary and mandibular right incisors and canines. During each session, 5 bites were completed by using a new standardized carrot sample for each bite. Maximum frequency (Hz) and peak-to-peak amplitude (mV) of the vibrations along the occlusogingival axis of the maxillary right canine were visualized and recorded ( Fig 2 ) with a digital storage oscilloscope (model 54601B; Hewlett-Packard, Palo Alto, Calif).
A range of clinically relevant archwire vibration characteristics was established by calculating the means (± standard deviations) and then subtracting and adding 1 SD to and from this mean. Hence, the mean vibration frequency was 98 (± 41) Hz with a range of 58 to 139 Hz, and the mean peak-to-peak vibration amplitude was 151 (± 39) mV with a range of 112 to 190 mV. These frequency and amplitude values were combined for a total of 9 clinically relevant vibration scenarios that were tested in vitro to simulate a comprehensive range of vibration scenarios.
For the ex-vivo portion of the study, an experimental apparatus was used to test the effects of vibration on frictional forces as 2 types of orthodontic brackets were retracted along a 0.017 × 0.025-in stainless steel archwire (Dentsply GAC International, Bohemia, NY) that was secured at both ends with retention bolts and washers ( Fig 3 ). The retention bolts were attached to an acrylic plate, which in turn was bolted to a large steel plate atop 2 cement columns. This secure mounting reduced the effects of extraneous vibrations. The testing area was maintained at 37°C to simulate intraoral temperature and measured with a digital thermometer.
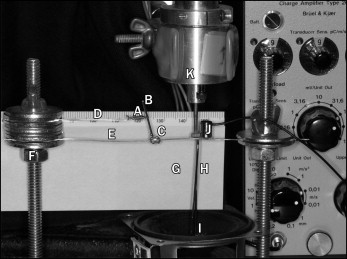
An impulse hammer constructed of 0.036-in-diameter stainless steel wire (Dentsply GAC International) bonded to a flexible diaphragm served as the vibration source and was positioned just below and in contact with the archwire ( Fig 3 ). Movement of the flexible diaphragm was generated by an electromagnet. A waveform generator (model 33120A; Hewlett-Packard) was used to input each of the 9 frequency and amplitude combinations into the electromagnet. Vibration of the archwire was measured by using the same piezoresistive accelerometer as used in vivo, and a linear differential transformer (7DCDT LVDT; Hewlett-Packard, Waltham, Mass) confirmed the amplitude of displacement ( Fig 3 ).
Two types of stainless steel brackets with 0.022 × 0.028-in slot dimensions for the maxillary right canine were compared. One type of bracket (DamonQ, 491-6480; Ormco, Orange, Calif) had a mesiodistal width of 2.9 mm and characteristics of passive ligation by closing a door and creating a tube to constrain the archwire. The other type of bracket (Unitek Victory Series, 017-880; 3M Unitek, Monrovia, Calif) had a mesiodistal width of 3.4 mm, conventional twin design, and characteristics of active ligation by using an elastomeric ligature (3M Unitek) to constrain the archwire. All ligatures were stretched once to approximately 3 times the original lumen size to simulate the elastic force decay that occurs in vivo. Five brackets of each type were tested at the 9 vibration scenarios.
Each bracket had bonded (Transbond XT; 3M Unitek) to its mesh pad a moment arm that was a 0.032-in-diameter stainless steel wire (Dentsply GAC International) that extended superiorly with a notch 10 mm above the center of the bracket slot ( Fig 3 ). This moment arm was perpendicular to the gingival and incisal walls of the bracket slot and parallel to the pulpal wall of the bracket slot. A mounting jig fixed atop standardized graph paper was used to ensure that the bonded moment arm was orientated the same for all 90 brackets.
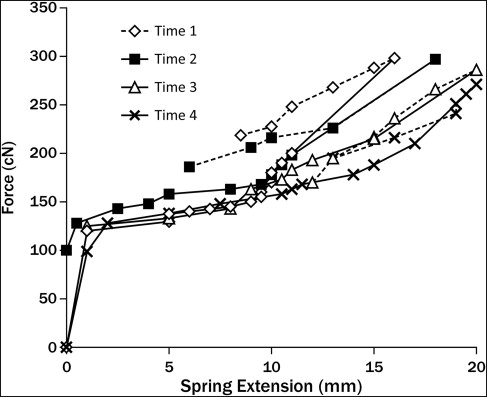
A nickel-titanium closed-coil spring (Dentsply GAC International) was extended from the notch in the moment arm to a hooked auxiliary wire that was parallel to the archwire below it ( Fig 3 ). This configuration produced a moment between the bracket and the archwire, mimicking intraoral canine retraction when a force is applied to a bracket hook located 10 mm from the tooth’s center of resistance. To characterize the moment produced, the spring was calibrated at 37°C to determine magnitudes and consistencies of forces delivered and the range over which the unloading forces were relatively steady. The manufacturer-reported spring force was 150 cN. Because variability in these reported values over clinically applicable deactivation ranges have been found, spring calibration was completed at 4 time points: before any trials and after 30, 60, and 90 trials. During calibration, the spring was held vertically with 1 end hooked to a stable bench-top extension arm, and the other hooked to a free-hanging container. Changes in spring length were measured while weights were incrementally added to the container until a maximum spring extension of approximately 18 mm was reached, and then decrementally removed until the spring extension returned to 0 mm.
The results of the 4 spring calibrations ( Fig 4 ) showed an average force of 146 cN and a range 128 to 178 cN, between 10 and 2 mm of spring extension during deactivation. The average force difference at 10 and 2 mm of spring extension over the 4 calibrations was 35 cN. Hence, on average, the moment associated with the experimental apparatus was 1460 cN-mm, which was deemed comparable with the magnitudes of moments produced clinically but opposite in sign.
Each bracket-moment arm unit was individually secured onto the archwire as previously described for passive or active ligation. Upon attaching the coil spring to the moment arm, the bracket-moment arm-spring complex was pulled along the horizontal archwire until the spring was activated 12 mm. The bracket was then released to come to rest at static equilibrium, the position where friction at the bracket-archwire interface could not be overcome by the force of the spring. At this point, the prescribed vibration was introduced into the system and the time (in seconds) for each bracket to be retracted along the archwire from 10 to 2 mm of spring extension was recorded as a measure of frictional resistance. The order of the 90 tests was randomized by using commercial software (Excel, version 2010; Microsoft, Redmond, Wash). New brackets and archwires were used for each test. All results were incorporated into the data analysis.
To measure accurately bracket movement, a millimeter ruler was mounted adjacent to the bracket-moment arm ( Fig 3 ), and a video camera was used to record each trial. For each bracket, frequency, and amplitude combination, video images were viewed frame-by-frame via commercial software (Windows Media Player 2010; Microsoft) to determine time-dependent changes in bracket position. Measurement bias was controlled by having 3 trained examiners (J.E.O. and 2 external examiners) view the video images and record bracket movements for each trial. All values from the 3 examiners were recorded and averaged to determine the time value for each trial. Furthermore, brackets that did not move the entire distance from 10 to 2 mm were assigned a maximum time value of 900 seconds, which was deemed to represent maximum frictional resistance in this study. Two weeks later, random trials were viewed to ensure reproducibility of the bracket movement measurements.
The ex-vivo tests involved 3 independent variables: vibration frequency, vibration amplitude, and ligation method. More specifically, low, medium, and high frequencies of 60, 100, and 140 Hz, and amplitudes of 110 (0.12 mm), 150 (0.16 mm), and 190 mV (0.20 mm) were used. Bracket ligation was passive or active as previously described. The dependent variable, bracket-archwire frictional resistance, was measured as a function of time for each bracket to move while subjected to the prescribed tipping moment.
Data and statistical analyses used backward linear regression to determine which, if any, independent variables had no significant effect on the dependent variable, bracket-archwire frictional resistance. The F test via a 2-factor analysis of variance (version 18.0; SPSS, Chicago, Ill) (α = 0.05) was then used to test for main effects and interaction effects of the remaining independent variables. If the omnibus test indicated significant differences in friction for the differing independent variables, the Ryan-Einot-Gabriel-Welsch F post-hoc analysis was used to assess pair-wise comparisons and allow for control of type I error.
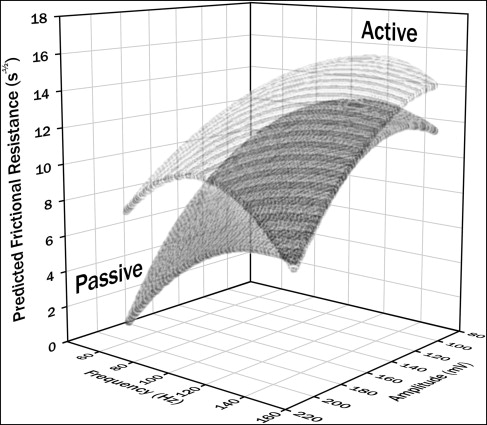
The predictive statistical modeling was applied to the ex-vivo experimental results to investigate expected frictional characteristics between the 2 bracket ligation types for a broader range of the frequencies and amplitudes of vibration. As a first step, Markov chain Monte Carlo full-data imputation (SAS Institute, Cary, NC) was used to create 5000 samples, and then averages from these samples were used to fill arbitrary missing values in the data from the 90 ex-vivo tests. Next, response surface regression was used to predict the variance seen in the original model for a larger sample set, data were normalized by the square root of time (s ½ ) transformation to meet the assumption of normality, and a lack-of-fit test indicated that the response surface models were adequate for both active and passive brackets. Canonical and ridge analyses showed that the response surface at the stationary point was maximal for both active and passive brackets ( Fig 5 ). These results were then used to create 3-dimensional response surface contour plots of predicted frictional resistance over a range of frequencies and amplitudes for comparison between bracket ligation types.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


