Chapter 9
When and How to Articulate
Aim
The aim of this chapter is to describe when and how to use an articulator.
Objective
After this chapter the reader will understand when an articulator is necessary in the provision of crowns.
Introduction
Articulating casts is time consuming and costly, but justified in certain cases. It is important to understand what type of articulator to use in these situations. In general, the provision of single restorations and cases in which the casts can be easily located into the ICP, do not need an articulator (Fig 9-1a–c).

Fig 9-1 (a–c) This patient has an intercuspal position which is difficult to record. Pencil marks record where the opposing teeth contact, providing sufficient information to articulate the models. For the construction of most single indirect restorations handheld casts are sufficient.
There are circumstances when the articulation of casts is important. These include:
-
reproducing lateral guidance (Chapter 7)
-
occlusal analysis, diagnostic wax-up and trial adjustments
-
extensive crowns and bridges with the loss of the intercuspal position.
A frequent question when restoring root-filled canines is: should the occlusion be restored to canine guidance or changed to group function? Converting the guidance to group function can protect the weakened tooth. Removing canine guidance can, however, lead to a short clinical crown with an unacceptable appearance (Fig 9-2). In these situations occlusal adjustment might be required to protect the weakened tooth.

Fig 9-2 This patient has a missing upper canine and the lower canine has overerupted. Avoiding heavy occlusal contact in lateral excursions would lead to an unacceptably short pontic. Orthodontic intrusion or adjustment of the lower canine will provide sufficient vertical space to replace the missing tooth. The same applies if the upper canine was compromised by a root filling and post retained core with no ferrule.
Occlusal Adjustment
Occlusal adjustment can be undertaken before preparation for a crown, or at the time the crown is fitted. Minor occlusal adjustments are often performed at the fit stage; however, the amount required is not always predictable. In cases in which extensive occlusal adjustment is necessary, this needs to be identified during the preoperative clinical examination. When fitting a crown, unplanned occlusal adjustment of opposing teeth is not good practice, and from a patient standpoint is seen to be an error of judgement. Planned occlusal adjustments should be practised on articulated study models. This allows the amount and nature of the adjustments to be fully appreciated and possibly explained to the patient prior to embarking on the necessary operative procedures. Exposure of dentine, during adjustments can lead to sensitivity and indicate coronal coverage. In extreme cases elective root canal treatment may be required (Fig 7-3, Chapter 7).
Number of Teeth Being Restored
Restorations placed in patients with group function rather than canine guidance need more clinical time at the fit stage. In these situations, articulated working casts reproduce the movements of the mandible and allow the technician to make all but the final adjustments in the laboratory. This reduces clinical time (Fig 9-3a,b).
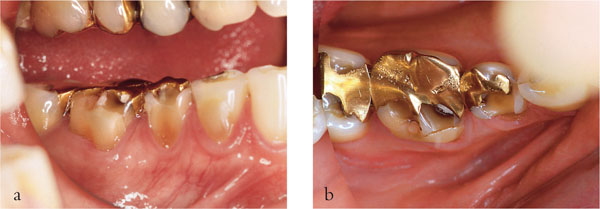
Fig 9-3 (a,b) The worn lower right premolar and molar teeth require replacement gold crowns. The patient has group function in lateral excursions. The use of an articulator will reduce chair-side time required for adjustment of the occlusion.
The necessity to articulate study and working casts increases with the number of teeth (units) to be crowned. As the number of prepared teeth increases, fewer teeth are available to locate the casts together in the ICP and the risk of errors increases. The choice of articulator type depends upon the clinical situation and complexity of the case. For example, if all the anterior teeth are to be crowned, preserving the anterior guidance, possibly with a custom-formed incisal guidance table requires a semiadjustable articulator (Chapter 7; Fig 7-11).
For crowns on more than one posterior tooth, the choice of articulator depends on the lateral guidance. Handheld, simple hinge or average value articulators are normally sufficient in cases with canine guidance, given disclusion of the posterior teeth in lateral excursion. Whereas, teeth involved in group function tend to require multiple adjustments in the laboratory, justifying the use of a semiadjustable articulator.
Reorganising the Occlusion
When all or most occluding teeth require new restorations, a reorganised approach is indicated. The occlusion is usually reorganised to the terminal hinge axis at a chosen occlusal vertical dimension. A semiadjustable articulator is necessary in such cases (see Chapter 7).
Types of Articulator
There are four main types of articulator, with increasing degrees of complexity.
Simple Hinge
This type of articulator consists of a simple hinge mechanism, linking the upper and lower casts (Fig 9-4). There is no relationship between the anatomical position of the condyles and the occlusal surfaces of the teeth. As a consequence, some adjustment of the cuspal inclines of the restoration may be needed on closure to compensate for the inaccuracy of the articulator. The adjusted crowns will tend to have cusps with reduced height and shallow angles, giving them a relatively flat appearance.

Fig 9-4 A simple hinge articulator.
Average Value
The condylar elements on the average value articulator (Fig 9-5) are not anatomically related to the occlusal plane of the teeth. Average value articulators provide lateral excursive and protrusive movements and have condylar inclinations set to an average value of 30°. The incisive guidance table is usually the only component that can be altered. This type of articulator finds few applications in fixed prosthodontics.

Fig 9-5 An average value articulator.
Semiadjustable Articulators
There are two types of semiadjustable articulators, the arcon (Fig 9-6a) and non-arcon (Fig 9-6b).
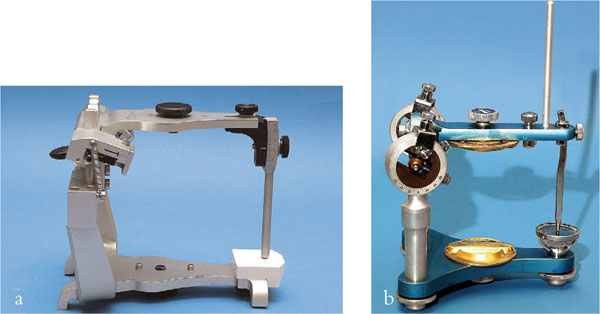
Fig 9-6 (a,b) Semiadjustable articulators. An example of an arcon articulator is illustrated in Fig 9-6a. The articulator shown in Fig 9-6b is a non-arcon articulator.
In the arcon design, the ball or condylar element is attached to the mandibular arm of the articulator and is anatomically correct. Non-arcon articulators have the condylar “ball” attached to the maxillary arm housed in a track connected to the mandibular component. Non-arcon articulators are anatomically incorrect, making it more difficult to appreciate the dynamics of movement of the casts.
A facebow record is normally used to mount the maxillary cast to the upper frame. An ICP or RCP occlusal record is used to mount the mandibular to the maxillary cast. This produces a close approximation of the anatomical relationship between the condyles and the occlusal plane of the teeth. Most semiadjustable articulators allow alteration of the condylar inclination, Bennett angle and movement, and incisal guidance (Fig 9-7).
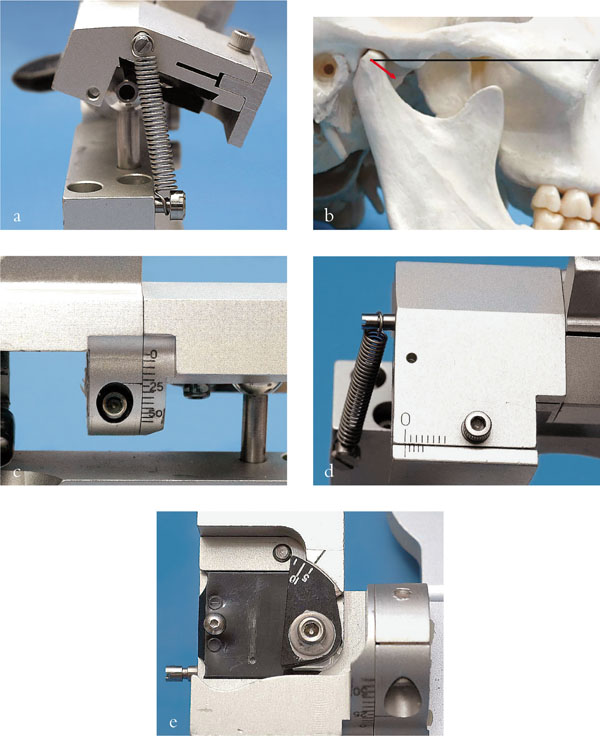
Fig 9-7 (a–e) Adjustable components on the Denar semiadjustable articulator. The lateral view of the condylar element of the articulator and skull shows the condylar guidance (a and b). This can be adjusted by the screw at the back of the articulator to the correct angle on the scale shown (c). Bennett movement (progressive side shift) can be adjusted by the small vernier scale on the top of the condylar element (d), and the Bennett angle (immediate side shift) on the inferior side of the condylar element (e). Intercondylar distance (c) and Fisher angle cannot be set as on the fully adjustable articulator.
Fully Adjustable Articulators (Fig 9-8a–c)
Fully adjustable articulators are very sophisticated devices, but are rarely used. A pantographic facebow records the terminal hinge axis, the position of the condyles and the movement of the condyles. In addition, more adjustments are possible than with a semiadjustable articulator, including changes to the intercondylar width and Fisher angle. Furthermore, condylar inserts can be used to duplicate the curved anatomy of/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


