Chapter 8
Generalised Gingival Ulceration
Aim
The aim of this chapter is to detail those clinical entities that may present as widespread or multiple areas of gingival ulceration.
Outcome
Having read this chapter, the reader should be able to formulate a differential diagnosis in cases of generalised gingival ulceration. They should be aware of the extra-oral manifestations of associated conditions and request and interpret those investigations that will assist definitive diagnosis so facilitating effective clinical management. Table 8-1 summarises the conditions discussed in this chapter.
| Major Categories | Sub Categories | Frequency of Condition | Management Setting |
| Mucocutaneous disease | Mucous membrane pemphigoid | Uncommon/rare | Referral to specialist units for treatment, monitoring and management of possible extra-oral manifestations. |
| Pemphigus | Rare | Referral to specialist units – this is a serious condition that may be life-threatening in some cases. | |
| Lichen planus | A common condition but very rarely produces generalised gingival ulceration. |
Severe recalcitrant cases should be referred for specialist assessment. | |
| Haematological | Leukaemias | Uncommon | The condition itself is clearly managed by haematologists. Oral hygiene measures can be undertaken in primary care. Management of the oral mucosal manifestations of chemotherapy/ radiotherapy should be managed in specialist units. |
| Lymphomas | Uncommon | As for the leukaemias | |
| Other haematological disease (e.g. myelosuppressive states) |
Rare | As for the leukaemias | |
| Infections | Primary herpetic gingivostomatitis – See Chapter 4 | Uncommon More usually associated with erythema than generalised gingival ulceration. |
Supportive measures and antiviral agents such as aciclovir which are only of real value if therapy is instituted at onset or very early in the course of the disease |
Vesicles and Bullae
A chapter specifically devoted to vesicular lesions cannot be justified, and therefore some pointers towards their investigation are provided briefly here. The most likely causes of gingival or mucosal vesicles are:
-
Viral infection
-
Trauma, which may be thermal, chemical or mechanical
-
Vesicullo-bullous disease such as mucous membrane (cicatricial) pemphigoid.
In the case of viral lesions, explore the history for a prodrome and check for lymphadenopathy (Fig 1-6) and pyrexia. If trauma is a cause this should be evident from the history, and fluid collected from the vesicle will be inflammatory in nature, with an absence of systemic signs of infection. Vesiculo-bullous diseases are dealt with in detail in Chapters 7 and 8.
Mucocutaneous Disease
Pemphigoid
Pemphigoid is an autoimmune vesiculobullous disease that manifests with subepithelial bulla formation as a result of the production of antibodies directed to the basement membrane zone of the epithelium. The disease is usually seen in patients over 50 years of age and is twice as common in females (Chan, 2002). There are two major variants of the condition:
-
Mucous Membrane Pemphigoid – predominantly mucosal involvement.
-
Bullous pemphigoid – predominantly cutaneous involvement.
Clinical appearance
-
The manifestations of mucous membrane pemphigoid often commence in the mouth and on occasions may be confined to the oral mucosa. (Fig 8-1).
-
Although oral lesions rarely precede skin lesions in bullous pemphigoid, oral mucosal disease may be a feature of this variant.
-
The main periodontal manifestation of mucous membrane pemphigoid is desquamative gingivitis (Fig 8-2), which may be the only oral feature of the condition (see Chapter 4). Shallow erosions may occur in desquamative gingivitis associated with vesiculobullous disease (Fig 8-3) (Richards, 2005).
-
Serum anti-basement membrane antibodies can be identified in 80% of cases of bullous and 60% of cases of mucous membrane pemphigoid.
-
Desquamative gingivitis may also occur in pemphigus/lichen planus/DLE.
-
Extra-oral manifestations of mucous membrane pemphigoid are problematical due to scarring and subsequent scar contraction. Common sites of involvement include the eyes, genitals and oesophagus.
-
Rarely there may be an association with internal malignancy.
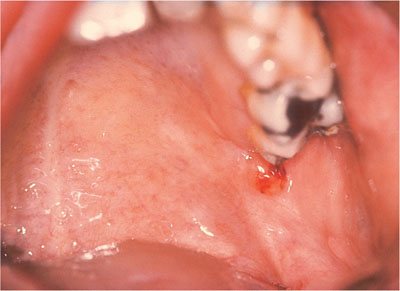
Fig 8-1 Small blood-filled blister that could be mistaken for a traumatic blister.

Fig 8-2 Mucous membrane pemphigoid presenting as desquamative gingivitis.

Fig 8-3 Desquamative gingivitis with erosions.
Clinical symptoms
-
Soreness is the principal symptom often accompanied by bleeding on brushing.
-
The discomfort may be such that the patient cannot tolerate flavouring oils used in many dentifrices.
-
Patients may also be concerned at the appearance of the gingivae, which may be fiery red.
-
Patients may complain of intra-oral blistering, but the blisters often go unnoticed. It is only when they burst to produce painful ulceration that the problem is drawn to the patient’s attention. The blisters may persist for several days, but often rupture within a few hours.
-
Blistering and subsequent ulceration may be provoked by the ingestion of abrasive foods.
Aetiology
-
Pemphigoid is an autoimmune disease associated with the production of antibodies to the basement membrane zone of the epithelium.
Involvement of non-gingival sites
-
Mucous membrane pemphigoid, as the name suggests, can affect any mucosal surface. Intra-orally the distal hard palate and soft palate are commonly affected as the bolus of food is pushed up into this location prior to deglutition. Clinically the appearance is one of shallow irregular ulceration, with an erythematous and sometimes haemorrhagic border (Fig 8-4). There may be keratosis peripheral to the ulceration representing scar tissue that frequently accompanies healing.
-
Extra-oral involvement may involve the oesophagus, which can become stenosed producing dysphagia.
-
Genital lesions – these may be very disabling.
-
Ocular lesions – these are often initially insidious and may affect up to 60% of patients. They are potentially serious, compromising sight. The eyelids may become sore as a result of blistering and subsequent ulceration. Subsequently the eyelids turn inwards due to scar contraction (entropion). Conjunctival scarring also occurs producing a symblepharon (scarring and fusion of the tarsal and bulbar conjunctiva) (Fig 8-5).
-
Nasal lesions may occur, manifesting as bleeding and crusting of the nasal mucosa.
-
Cutaneous involvement may occur in mucous membrane pemphigoid.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


