Working with Dental Office Documents
LEARNING OUTCOMES
• Describe how to implement HIPAA regulations in the dental office record management system.
• Identify the types of records maintained in a dental office.
• Categorize the various types of records.
• Distinguish between active and inactive records.
• List the components of a clinical record.
• Describe the function of the components of a clinical record.
• Explain the rules for data entry on patient records.
• Explain the use of symbols and abbreviations in clinical records.
• List the components of patient financial records.
• Identify the various types of employee records.
Although every dental professional dreams of a paperless office, an office cannot operate without records. Thus when reality strikes one generally concludes that it is not possible to achieve this longed-for dream. There is also the human nature side of a potential paperless office. Some dentists could easily manage with a totally paperless office and yet there are those who must have a paper record to hold onto for each activity.
The dental office is inundated with a plethora of records and forms, all needed as part of the total dental business practice. These records are kept so that the people in the office can refer to the information later or use it to complete another task. A records management system will help store and retrieve records efficiently and keep the files current. The administrative assistant is required to maintain clinical, financial, employee, state, and federal records. Failure to perform any of these tasks can be a costly experience for the dental practitioner. Therefore, the administrative assistant who can pay routine special attention to detail in maintaining all types of records becomes an immeasurable asset to the dental practice.
HEALTH INSURANCE PORTABILITY AND ACCOUNTABILITY ACT
The Health Insurance Portability and Accountability Act (HIPAA) of 1996, which became effective immediately in the medical community but did not affect dentistry until April 2003, has significantly affected the dental profession in a number of ways.
Administrative simplification provisions of the Health Insurance Portability and Accountability Act of 1996 (HIPAA) have affected the dental profession. These provisions require national standards for electronic healthcare transactions. Dentists who transmit health information in an electronic transaction are required to use a standard format. Plans and providers who do not use electronic standards can use the Employee Retirement Security Act (ERISA) healthcare clearinghouse to comply with the requirement. Providers’ paper transactions are not subject to this requirement. Primarily the most affected area in the dental office is the area of transmission of dental claim forms, which is reviewed in Chapter 14. However, as one begins to study the management of patient records, the impact of privacy is one of primary concern.
HIPAA laws may seem daunting at first. However, the purpose is to protect and enhance patient rights; therefore, it is a positive action because everyone is a patient at one time or another. Protecting health information is the right thing to do, and it promotes safe practice for everyone on the dental team, especially the patient. It is also good risk management, helping each dental professional to prevent potential litigation. Security regulations, which the Department of Health and Human Services released under HIPAA, were conceived to protect electronic patient health information. Protected patient health information is anything that ties a patient’s name or Social Security number to that person’s health, health care, or payment for health care, such as radiographs, charts, or invoices. Each dental professional should become familiar with state as well as federal laws, as these laws are often more stringent than federal laws.
The American Dental Association (ADA) and most state dental associations have done an excellent job of providing its members with the necessary tools for the implementation of HIPAA. The ADA and state dental associations as well as many dental office stationers provide a HIPAA Security Tool Kit as shown in Figure 7-1. This kit contains most of the forms needed for privacy practices, including the following:
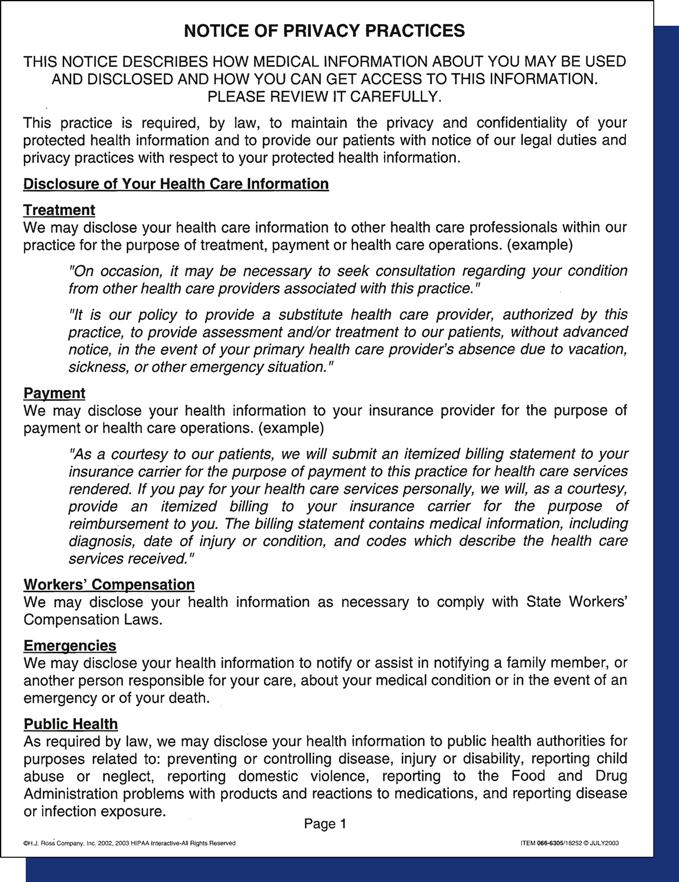
• The Notice of Privacy Practices form (Figure 7-2) presents information that the dental professional is required to give patients regarding the office’s privacy practices. This form may need to be changed to reflect the dental practice’s particular privacy polices or stricter state laws. The name of the practice may be on the notice, and it must be given to each patient at the date of the first service. In addition, the notice may be posted in a clear and prominent location in the office that is visible to any patient seeking service. Boxes 7-1 and 7-2 provide checklists for managing the privacy and security of patient records.
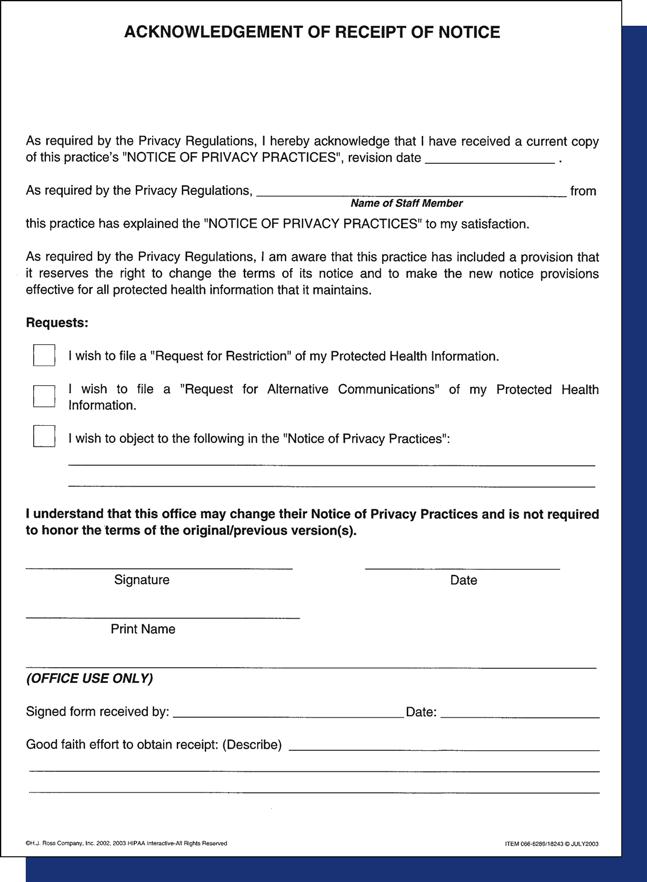
• Acknowledgement of Receipt of Notice of Privacy Practices (see Figure 7-3 on p. 100) is the form the patient signs to acknowledge that he or she has received a copy of the Notice of Privacy Practices. If the patient refuses to sign the form, the administrative assistant can indicate that an attempt was made to have the patient sign in the in-office section on the form. The patient may also opt to sign a separate refusal form that may then be placed in the record.
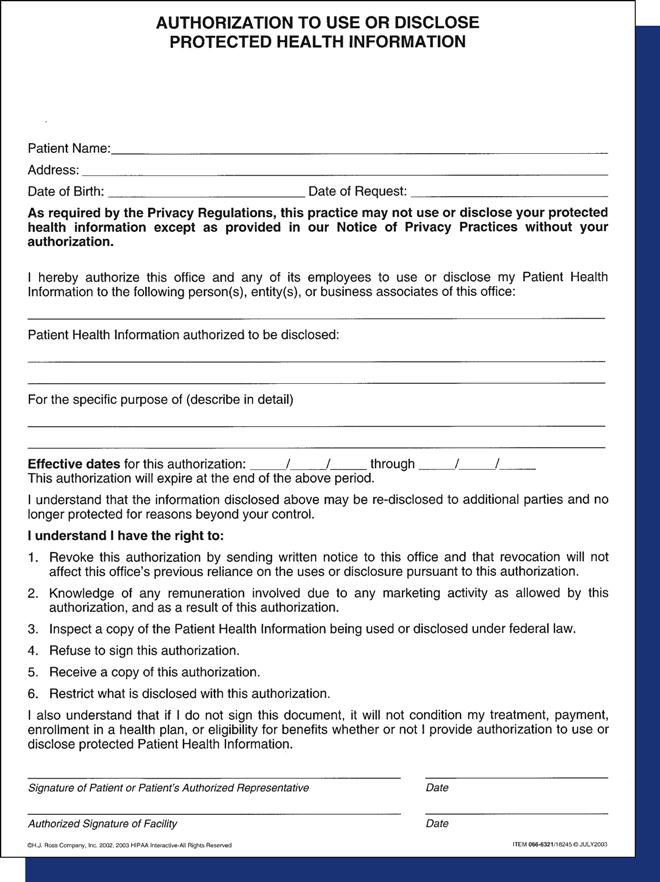
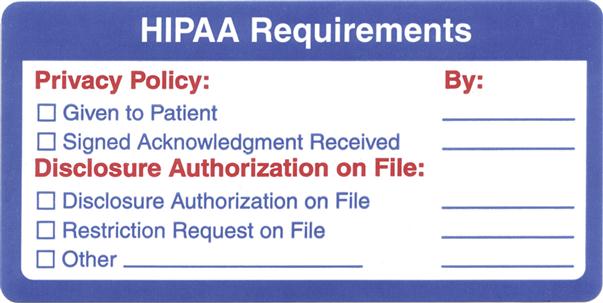
• Business Associate Contract Terms is a contract form that satisfies the obligation under the HIPAA and its implementing regulations issued by the U.S. Department of Health and Human Services (see Figure 7-4 on p. 101). This form ensures the integrity and confidentiality of protected health information that a business associate may create or receive for or from the dental practice. Other forms such as the Health Information Access-Response/Delay, Complaint, and Staff Review of Policies and Procedures, are available in the ADA manual or from the state dental society. In order to ensure that records are maintained for patients, a preprinted chart label can provide information about important HIPAA information for patient files (see Figure 7-5 on p. 101).
OVERVIEW OF A RECORDS MANAGEMENT SYSTEM
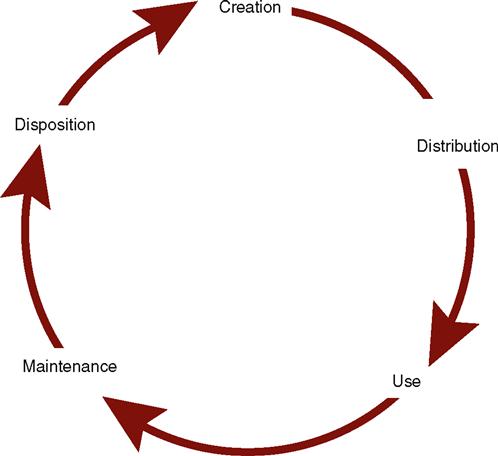
A dental office operates on information; it is created, processed, stored, printed, and distributed in many forms to various sites. Therefore, the dental administrative assistant must establish a logical, functional system for storing and retrieving information. A record is data in forms such as text, numbers, images, or voice that is kept for future reference. In a dental office this comes in the form of clinical, financial, radiographic, and photographic forms. Records management or an information management system refers to a set of procedures used to organize, store, retrieve, remove and dispose of records. Records have a life cycle, which begins with inception and ends with disposition (see Figure 7-6 on p. 102). The life cycle proceeds as follows:
 Practice Note
Practice NoteRecords have a life cycle that begins with creation and ends with disposition
CATEGORIES OF RECORDS
The administrative assistant must decide which records to keep, how to organize and store them, how long they legally must be retained, and when to dispose of them. In general, records can be categorized as vital, important, useful, or nonessential, and as active or inactive.
Vital Records
Vital records are essential documents that cannot be replaced. These include patient clinical and financial records and the office’s corporate charter and deed, mortgage, or bill of sale. These records should be kept in a fireproof theft-proof vault or safe, and copies often are kept in a protected, offsite location.
 Practice Note
Practice NoteVital records are essential documents that cannot be replaced.
Important Records
Important records are extremely valuable to the operation of the office, but they are not vital. They include accounts payable and receivable, invoices, canceled checks, inventory and payroll records, and other federal regulatory records. Such records may be needed for a tax audit or if a question arises about a financial transaction. Important records generally should be retained for 5 to 7 years. Most offices keep them for about 7 years or in accordance with federal or state regulations.
Useful Records
Useful records include employment applications, expired insurance policies, petty cash vouchers, bank reconciliations, and general correspondence. This category is difficult to define, because one office may consider a document useful, whereas another might find it indispensable. These records usually are retained for 1 to 3 years. Before discarding a document, it is always wise to check with the dentist or other staff members to see if it is still needed.
Nonessential Records
Nonessential records are the documents that lie around, have little importance, and take up space. They include such items as notes to you, reminders of meetings, outdated announcements, and pamphlets. Common sense dictates when these materials may be discarded.
TYPES OF PATIENT RECORDS
Patient records generally fall into two categories, clinical and financial. A recall system is another type of record that is retained separate from the clinical chart but that could be considered a type of clinical record. Clinical records are reviewed in this chapter; financial records are discussed in Chapter 15.
Clinical Record
The clinical record is a collection of all the information about the patient’s dental treatment. Although each patient’s clinical record is used during dental treatment, updating and maintaining this record is the administrative assistant’s responsibility. Success in maintaining clinical records requires cooperation and efficiency from each member of the dental healthcare team.
Accurate clinical records are vital for several reasons, as follows:
A patient’s clinical record commonly has the following components:
• Patient file envelope or folder
• Health history and update forms
• Clinical chart or examination form
• Dental diagnosis, treatment plan, and estimate sheet
• Medication history and prescription forms
• Consultation and referral reports
• Letters
Bulkier materials, such as diagnostic models, generally are stored in an area other than the business office. A cross-reference on the patient record makes these materials easier to locate. Although the dentist chooses the components of the clinical record, staff members’ opinions are important when selecting the forms because the staff members must maintain them. With more dental practices moving toward computerized systems, patient records and files are changing. More of the data will be stored in the computer, and the need for paper copies of these documents will decline.
Patient File Envelope or Folder
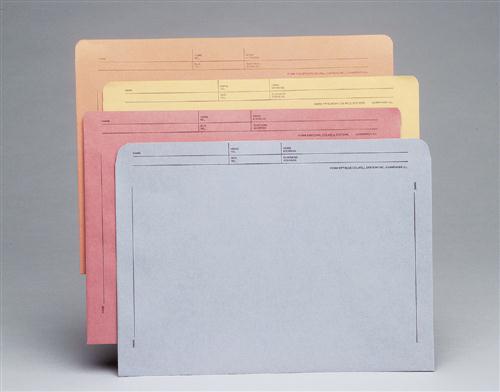
In most dental practices, use of an 8½ × 11-inch file envelope or folder guards against misplacement of records. In practices in which patients are seen by the dentist only or do not return on a regular basis, such as in an oral surgeon’s office, a smaller envelope (5 × 8 inches) may be desirable, or the envelope may be eliminated. File envelopes may be plain or color-coded. They are supplied in a preprinted format with spaces for patient information, including the patient’s name, address, and telephone number (Figure 7-7). This type of envelope is widely used and satisfies the needs of many practices.
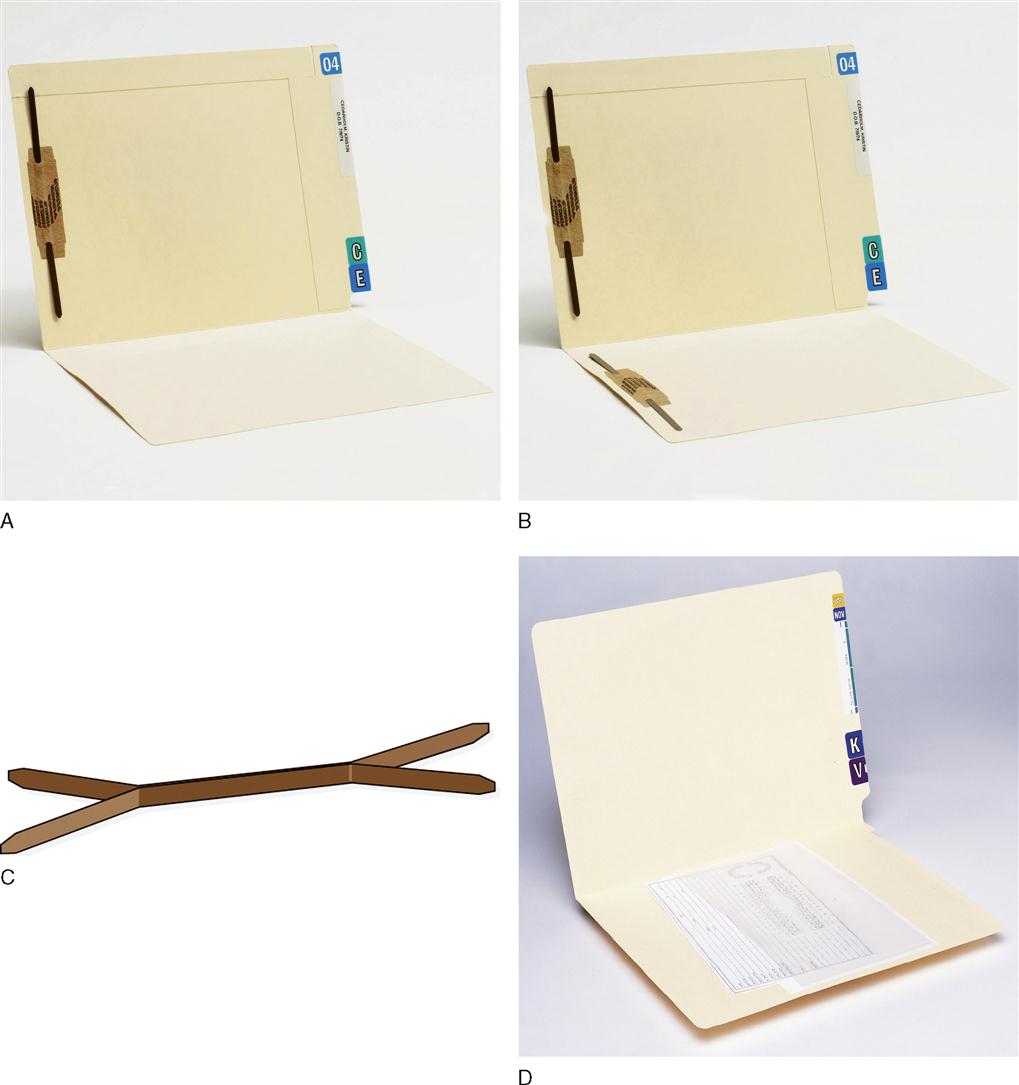
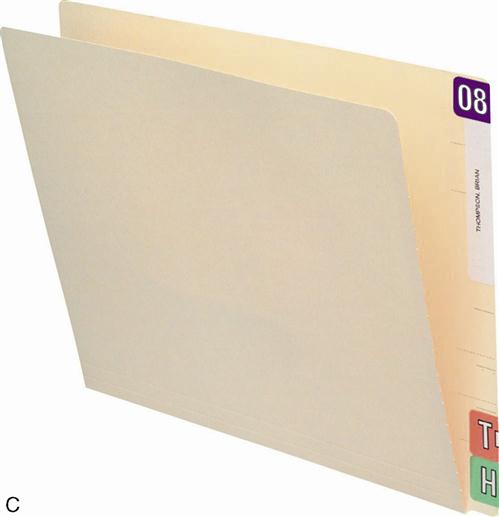
Another very common type of storage for patient records is an end-tab file folder with one or two two-hole fasteners (Figure 7-8 A,B). This type of folder requires the use of vertical-style records. The folders generally have a reinforced tab for easy label placement. They also are precut for quick insertion of a two-hole file fastener. Options include folders with pockets and diagonal cuts and expandable folders. Other auxiliary aids for these records include the hole punch, perm-clip fasteners, and polyvinyl pockets to hold small materials such as radiographs and CDs (see Figure 7-8 C,D).
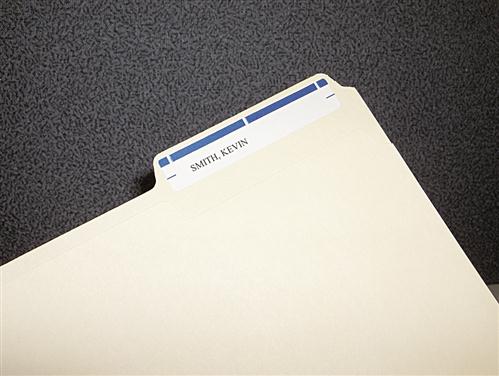
Whether folders or envelopes are used, some form of color-coding is necessary to make sorting, storing, and retrieval easier. Color-coding can be done as an alphabetical system or, in a group practice, can be categorized by dentist. In addition to the traditional label (Figure 7-9), either an alpha or numeric label system can be used to sort the records. Year aging labels can be used to identify inactive patient records that may need to be purged from the active storage system (Figure 7-10 A,B). In Figure 7-10, C, the letter T is the first letter of the patient’s last name, and H is the first letter of the patient’s first name. The two-digit number indicates the year of the patient’s last visit to the office.

Patient Registration and Health History Forms
Although they are often combined, these two forms contain two different types of data. They should be retained because they provide more detailed information about the patient. Stock forms are available from dental forms suppliers. Custom forms can be designed by most companies and these will address the special needs of the office. Some forms are available to address questions such as, “May we leave a message on you’re answering machine at the phone number you have given?” or “May we contact you at a cell phone number or text message you?” If there are other questions desired for the office, talk with the supplier and for a nominal price these can be modified to meet the office’s needs. Most supply companies provide patient forms in English and Spanish versions for use in various areas of the country. Many offices with Spanish-speaking patients have both forms available.
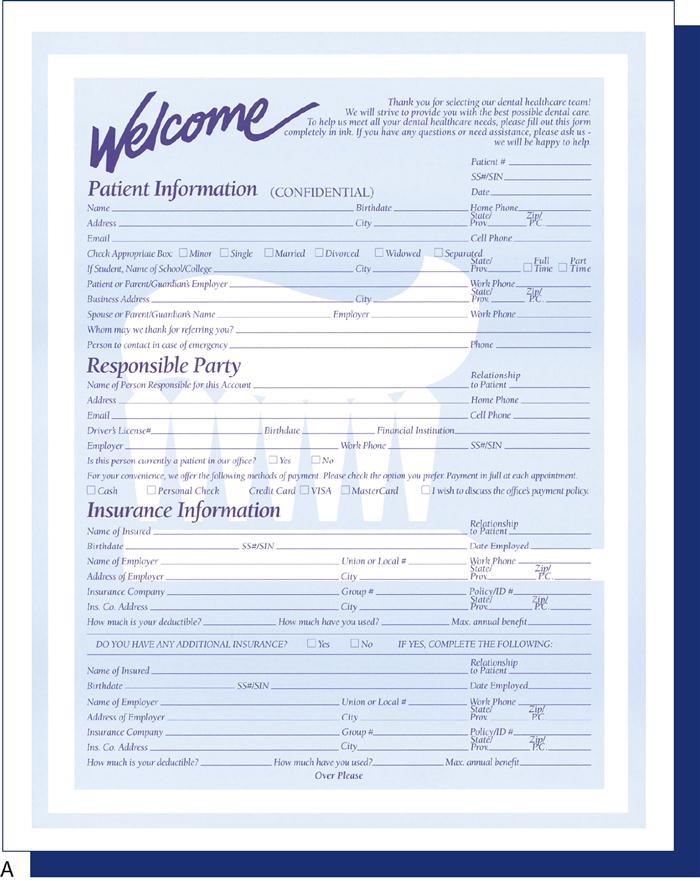
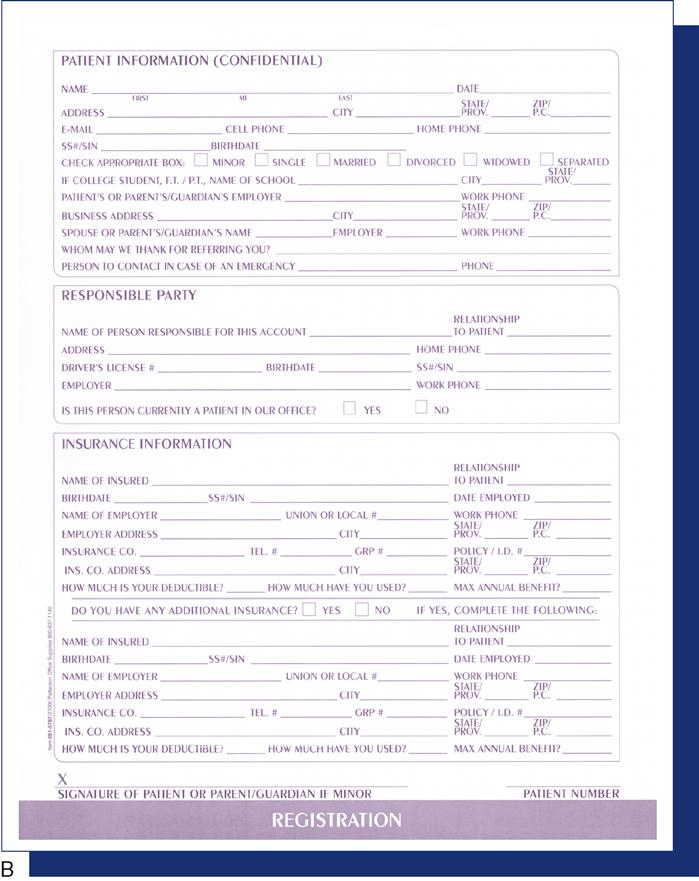
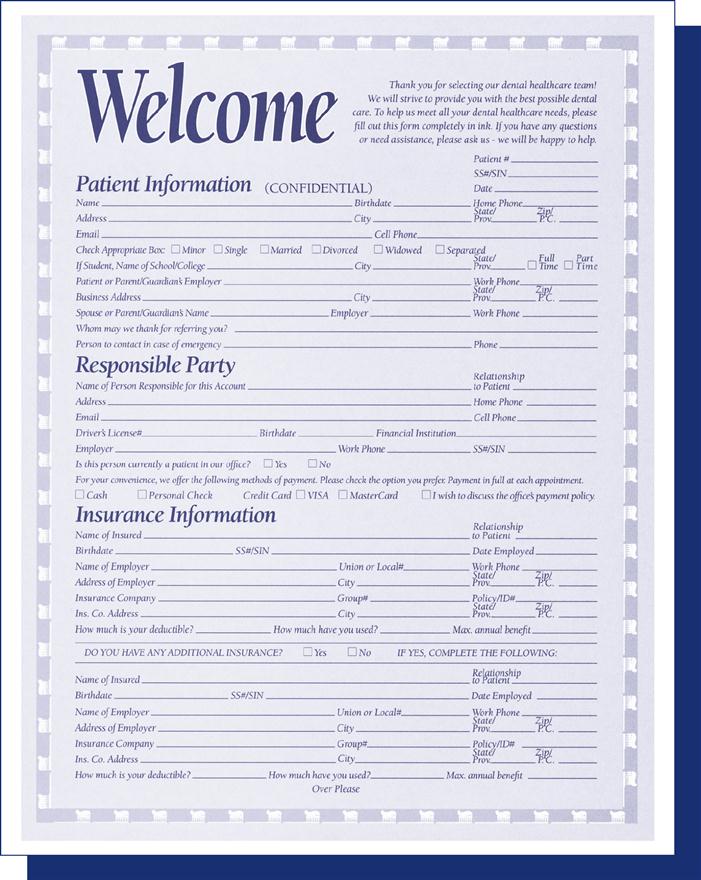
The patient registration form contains general information such as addresses and telephone numbers, as well as employment and insurance information. Figure 7-11 on p. 105 presents two common types of registration forms. This form enables the staff members to become better acquainted with the patient and can provide information for third-party payments and credit checks. Incomplete information on this form can complicate account collection later. Experienced business managers know that an account properly opened is half collected.
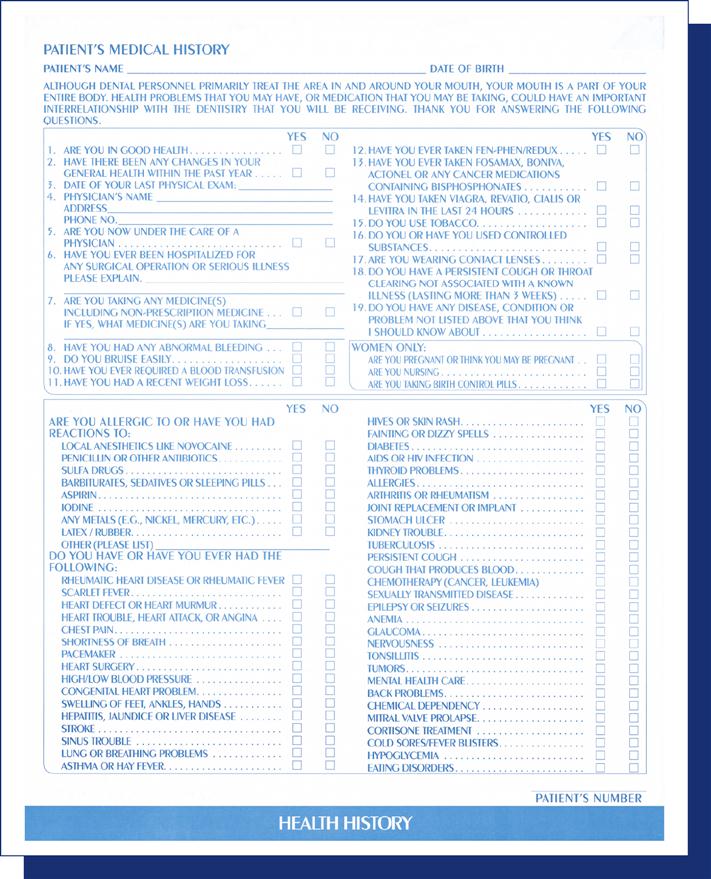
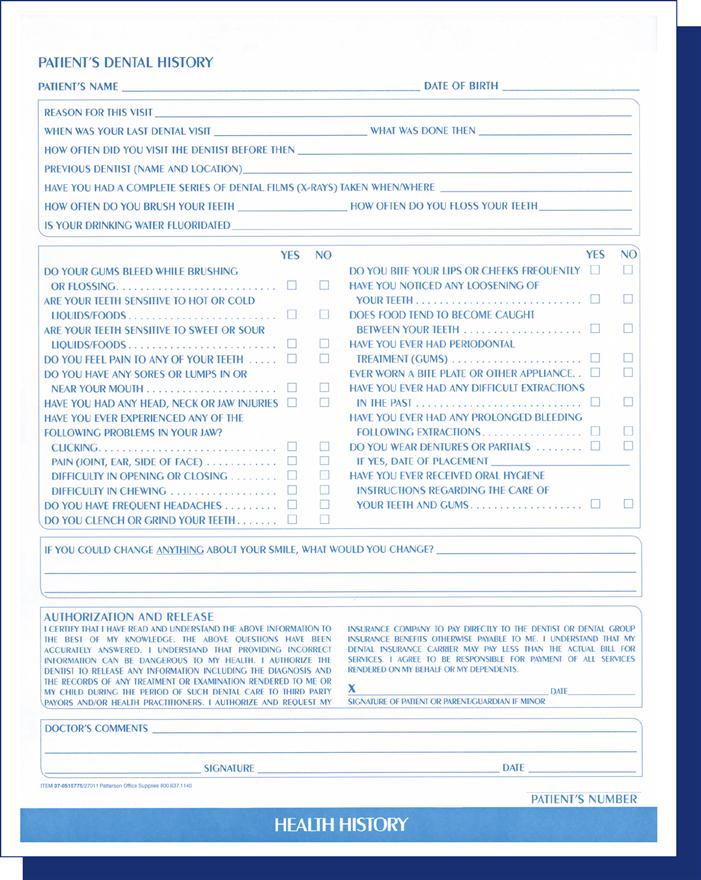
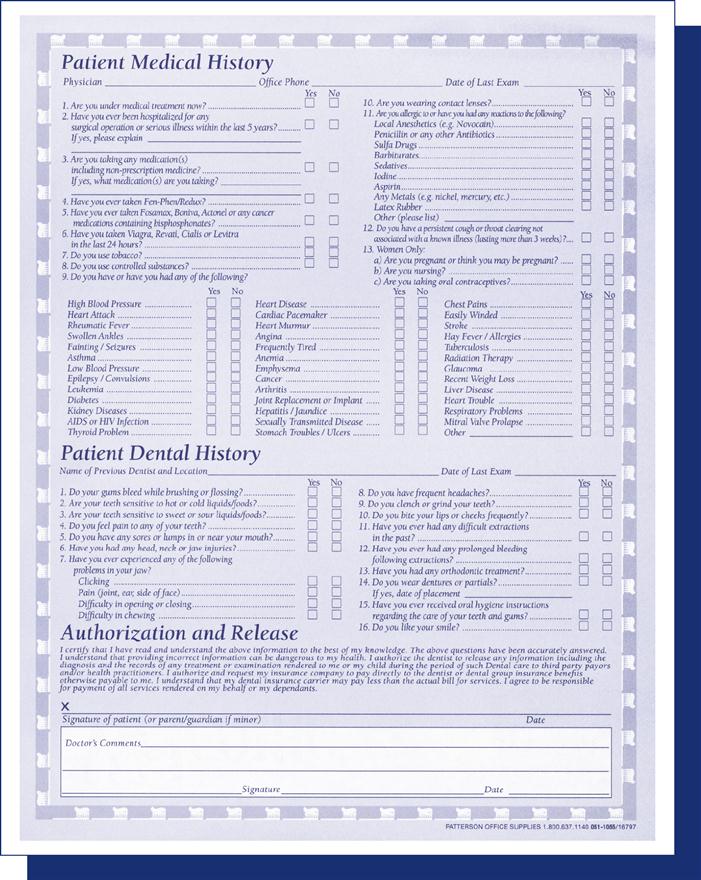
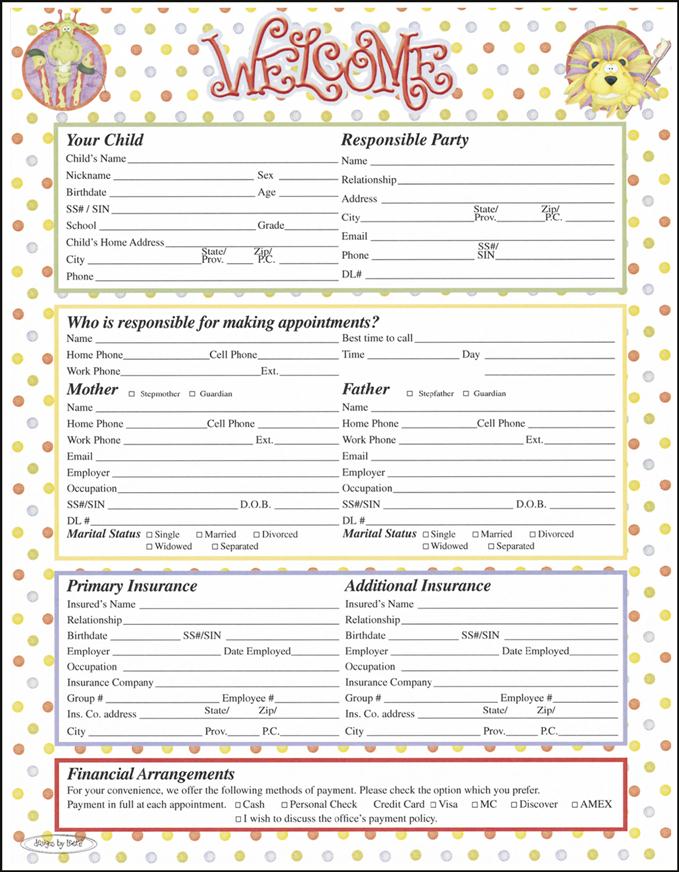
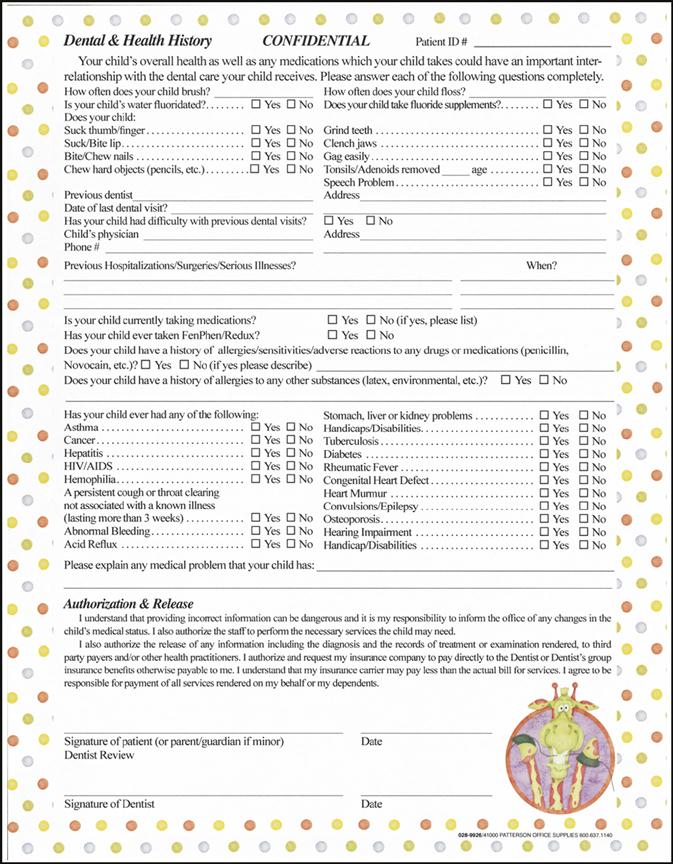
Each patient should fill out a health history form (see Figure 7-12 on p. 106) and date and sign it. If the dentist prefers to ask these questions in person, the patient should verify the answers recorded and sign the form. Figure 7-13 on p. 107 shows a combination health history and adult registration form. Figure 7-14 on p. 108 shows the pediatric version of this form. With children, the health history form should be completed by a parent or guardian, not by the child or a baby sitter. Make sure no nicknames are used and that all data are accurate, because this information is used later to complete insurance forms.
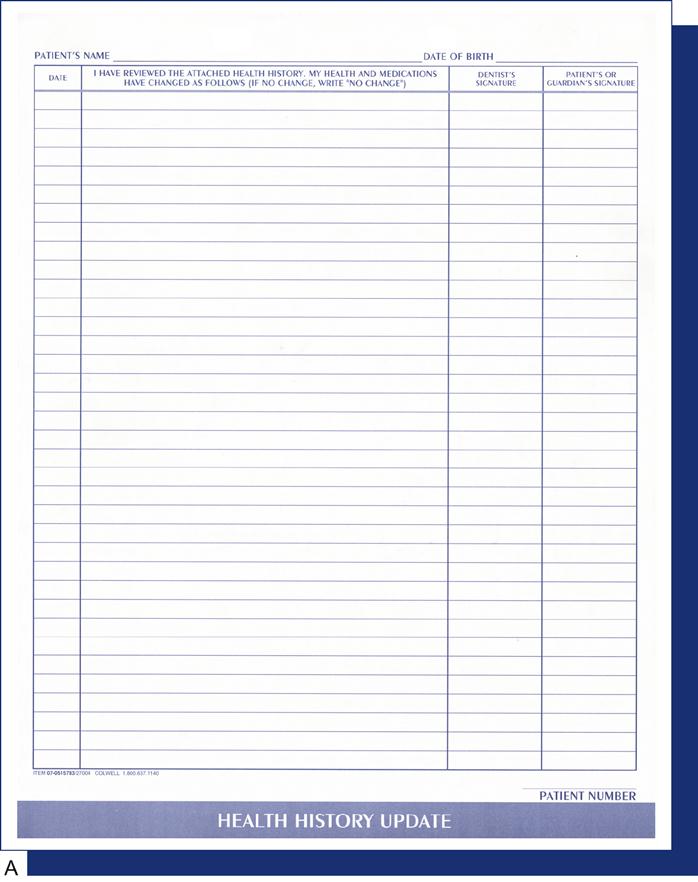
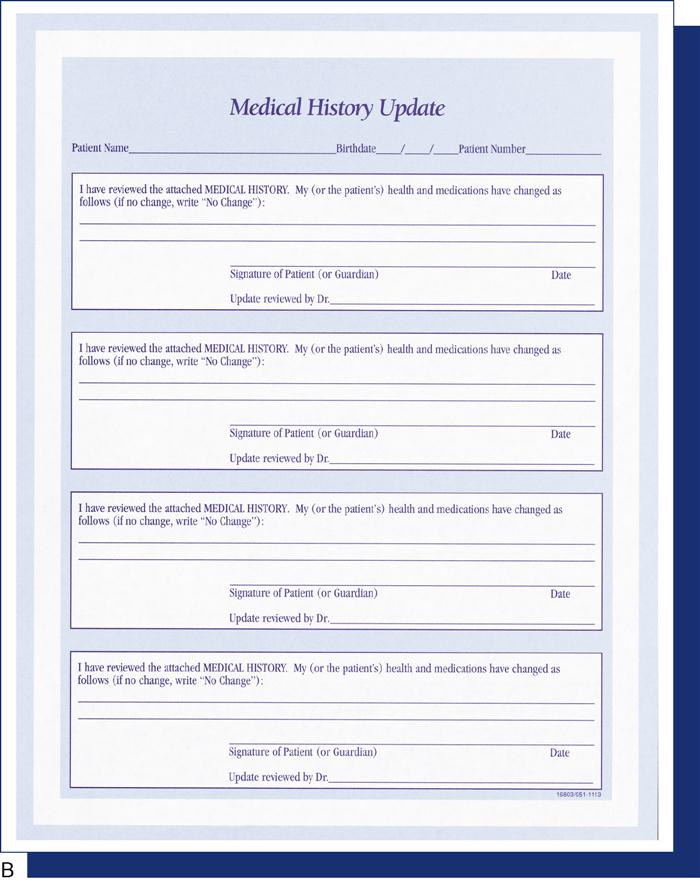
The patient’s history should be reviewed when the person returns for treatment if several months have elapsed since the last visit. A health history update form should be completed periodically to keep both the health history (see Figure 7-15, A on p. 109) and the personal information (see Figure 7-15, B on p. 109) current. The patient should sign and date this form.
Many types of patient registration and health history forms are available. For example, the form in Figure 7-16 on p. 110 can be used for children. Figure 7-17 on p. 111 shows a short-form style, which combines an abbreviated patient information form and health history form, which may be used for a transient patient. Regardless of the form used, it is important to remember that a current, accurate health history serves as a preventive measure in patient treatment and as a defense in malpractice suits. When collecting/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


