CHAPTER 7 SURGICAL ANATOMICAL CONSIDERATIONS FOR DENTAL IMPLANT RECONSTRUCTION
 Maxilla
Maxilla
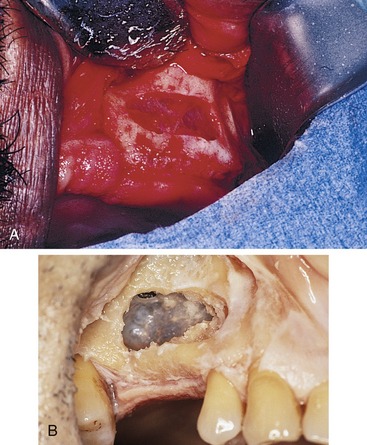
The maxilla is a hollowed and cuboid-shaped paired bone with its pyramidal base facing medially and separated by the nasal fossa. Its septum is in the center, bordered inferiorly and bilaterally by the oral cavity (Figure 7-1). These borders form the outer limits of the maxilla. The hollowed maxilla is covered by a three-layer mucoperiosteum lining known as the schneiderian membrane or sinus membrane with a thickness that varies between 0.3 and 0.8 mm.1 This membrane is in intimate relationship with the periosteum. Its color when healthy may vary from red to purple (Figure 7-2), and it has an elastic consistency. These membranes appear very thin, yellowish, and extremely friable in smokers. Most of the time, the maxillary antroplasty procedures for bone grafting and implant placements are limited to or aborted during surgery because of unrepairable membrane perforation. The branches of the maxillary nerve provide innervation of the maxillary sinus membrane. These include the superior alveolar branches of the infraorbital nerve, the greater palatine nerve, and the posterolateral nasal nerve. These nerves control the discharge of the mucous glands within the schneiderian membrane. The maxillary and facial arteries provide the main blood supply to the maxillary sinus. Venous drainage occurs either anteriorly or anterosuperiorly by the anterior facial vein into the jugular vein or posteriorly by vessels of the maxillary vein. The volume of the maxillary sinus may vary from 9.5-20 mL as reported by Alberti, with an average capacity of 14.75 mL.2,3
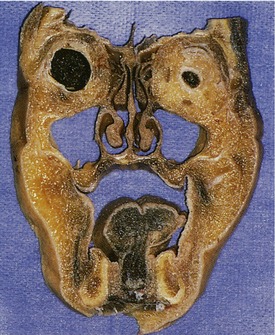
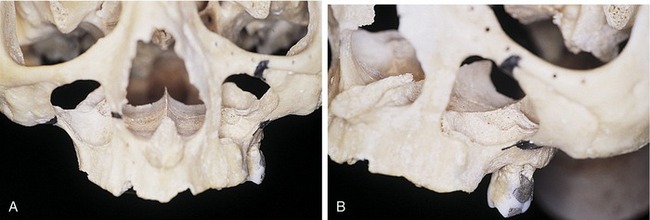
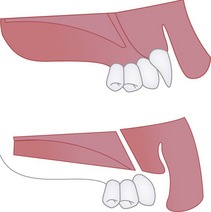
In normal conditions, the maxillary sinus maintains a close relationship with the alveolar ridge associated with the second premolars and first molar teeth. Roots of the first and second molars are often found in the maxillary antrum (Figure 7-3). Therefore when teeth are lost, the maxillary sinus tends to expand into the remaining residual alveolar bone because of the lack of functional stimulation by the teeth and the negative pressure during inspiration. Over time, pneumatization may cause the residual alveolar bone to resorb as a result of continuous expansion of the maxillary sinus along with horizontal and vertical forces (Figure 7-4). When maxillary sinus antroplasties are indicated to increase the width and height of the bony ridge, the sinus membrane usually is not torn because of its elasticity (Figure 7-5). In fact, the periosteum (membrane) is manipulated with surgical instruments in order to augment the antrum with bone graft materials of choice. In edentulous severely resorbed maxillas, the floor of the sinus is often the crest of the residual alveolar ridge and the bone level may approximate the level of the floor of the nasal cavity (Figure 7-6).

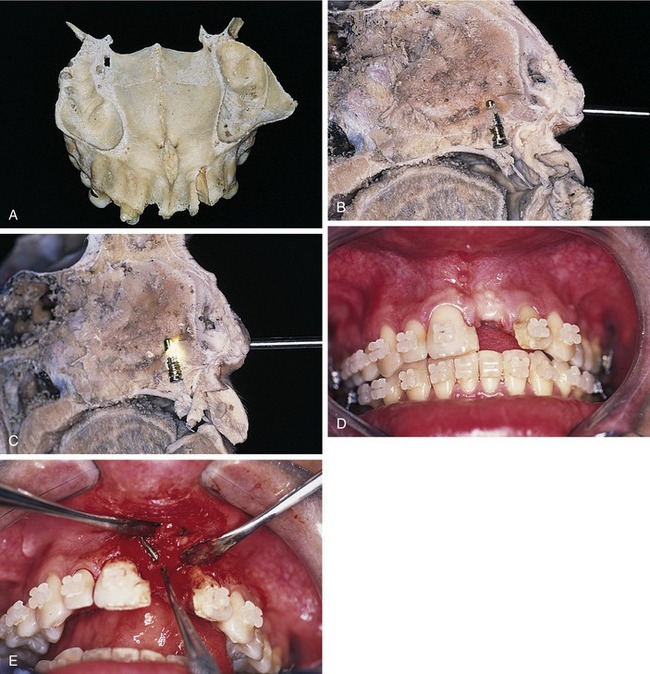
Figure 7-3. Horizontal cut of the maxilla shows the apex of the buccal roots of the molar in the right maxillary sinus.

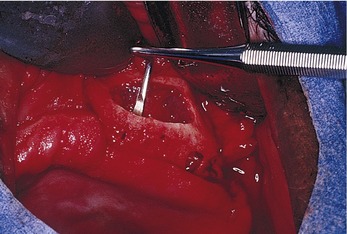
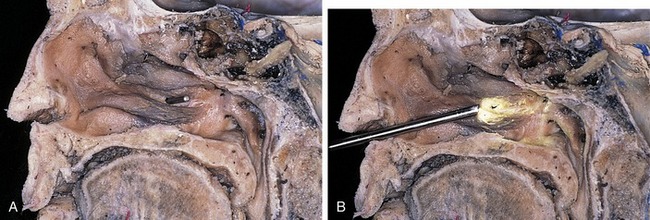
Figure 7-5. Elevation of the right maxillary sinus membrane for augmentation bone grafting procedure.
In an isolated study, it was found that the inferior turbinate is located 5 to 9 mm above the nasal floor (Figure 7-7).3 It is also known that when maxillary antroplasties are performed, bone grafting should be constructed vertically to 2 mm superior to the longest implant possible, which may be a minimum of 15 mm. Therefore the bone graft materials should be kept clear of this area to avoid blockage of the ostium.
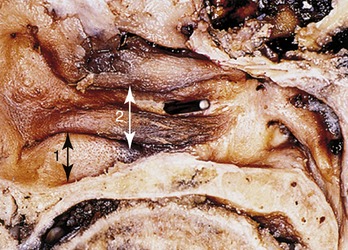
Figure 7-7. Cadaver specimen illustrates the distance between the nasal floor and the inferior turbinate.
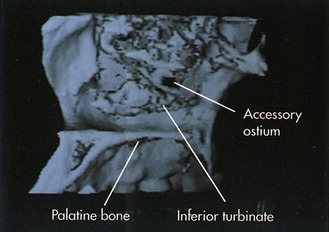
An accessory ostium, which occurs in 30% to 40% of all sinuses, is most likely to be found between the lower and middle turbinates (Figure 7-8). With these data and rationale, it follows that in extremely resorbed maxillas in which the floor of the sinus is level with the floor of the nose, it is wise to identify anatomic structures via nasal endoscopy and locate the existence of any accessory ostium (Figure 7-9), as well as its relation to either the sinus or nasal floor. Nasal endoscopy as a preoperative diagnostic tool will allow the identification of potential complications with antroplasty bone grafts before obliterating the accessory ostium or contaminating the bone graft, which may fall into the nasal cavity if proper precautions are not taken. The authors of this text advocate that in sinus elevation, a diagnostic endoscopy under topical anesthesia may be beneficial.
When placing an implant in the anterior maxillary region of resorbed maxillas, caution must be taken with respect to the incisive foramen that might be found close to the remaining alveolar crest (Figure 7-10).



The incisive canal is found adjacent to the nasal septum (Figure 7-11), 8-18 mm behind the anterior aspect of the floor of the nasal fossa. The nasal septum marks the upper end of the incisive canal, which contains the terminal branches of the nasopalatine nerve, the greater palatine artery, and a short mucosal canal (Stensen’s canal).4 The incisive canal has a length of 8-26 mm, measured from the oral cavity in adults. The axis of the canal forms an angle between 57 and 89.5 degrees with a plane through the eye and ear (Figure 7-12).4
Clinicians must develop a three-dimensional view of these bone structures and must understand that dangerous zones may appear when bone is lost vertically and horizontally. Implant placement may lead to failures if basic prosthetic principles are not applied and considered during treatment planning. A final consideration about the maxillary sinus refers to the oxygen concentration within the antrum, which is approximately 19%, falling to 9% when the true ostium is closed.5,6 The mean temperature inside the maxillary sinus is 31° C during inspiration and 37° C during expiration.4,7 If the true osti/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


