CHAPTER 7
Orthodontic Appliances
The introduction of fixed appliances to the teeth with bands or brackets set a milestone in the discipline of orthodontics. Orthodontic treatment options increased significantly; moreover, three-dimensional (3D) control of tooth movement became a standard goal of orthodontic treatment. Contemporary fixed appliances now have incorporated first-, second-, and third-order prescriptions. Numerous attachments and/or auxiliary appliances can now be attached to the fixed appliance, hence the term fixed-removable for such appliances as the headgear, removable transpalatal arch, and removable lingual arch. Fixed appliances, which encompass the various designs of brackets (directly bonded to enamel or laser welded to bands and cemented to teeth), tubes, buttons and others, with the activated arch wires in place, move teeth into new positions. Orthodontics reached out to industries with requests for “space-age” and biocompatible materials to facilitate and enhance treatment options. It is thus not surprising that the discipline went from the large gold bands and wires of Dr. Angle to the small, esthetic appliances constructed from various materials, including stainless steel, titanium, and ceramic, as well as combinations of the noted materials. In addition, arch wires that exhibit amazing memory and heat-activation characteristics have become the order of the day.
The amazing bracket designs comparable to classic art work and the highly developed arch wires have changed orthodontic treatment from laborious and time consuming to a very refined, efficient, and reliable practice; this is truly a remarkable ingredient in providing quality of life to millions of patients.
The development of the fixed appliance over the last 100 years incorporated sophistication second to none. The purpose of this chapter is to provide insight into these developments and stimulate further study by providing a brief overview of fixed orthodontic appliances.
1 What is a fixed orthodontic appliance?
A fixed orthodontic appliance has the capability of being fixed to teeth. Its design dictates either direct fixation by bonding to the enamel surface with composite cement or cemented via a band around the crown of a tooth. The nature of the appliance prevents removal by the patient, except if it is a fixed-removable appliance such as a headgear. The arch wires are then fixed to the brackets or tubes by clips, steel ligatures, or elastomeric o-rings to form the total fixed appliance and when activated leads to tooth movement.< ?xml:namespace prefix = "mbp" />
2 What characteristics should fixed orthodontic brackets or appliances exhibit?
Fixed orthodontic appliances or braces, commonly referred to as orthodontic brackets attached to teeth, should exhibit the following properties:
3 When and by whom was the edgewise appliance introduced to the discipline of orthodontics?
The appliance was introduced by Dr. Edward Hartley Angle in 1928.
4 Which appliance preceded the edgewise appliance?
The Angle System (
5 Why did Angle develop the pin and tube appliance?
Angle realized that the axial inclinations of teeth needed to be corrected. He developed the pin and tube appliance to enable orthodontists to accomplish root movement (
6 Which appliance did Angle develop in 1915 to replace the cumbersome pin and tube appliance?
The ribbon arch appliance (
7 Which modern appliance is based on the Ribbon Arch appliance?
The Begg appliance of Dr. Raymond Begg uses the vertical bracket slot principle; however, the bracket is upside down with the arch wire inserted from the gingival aspect and then held in place with a variety of pins. Each pin fulfills a different function (
FIG 7-4 The Begg Appliance in Stage 3; this stage uses various springs. The uprighting springs as shown allow for correct tooth inclination. Note that these are inserted in the vertical slot of the bracket and the arch wire is inserted gingivally.
(From Begg PR, Kesling PC: Begg orthodontic theory and technique, edition 2. Philadelphia: WB Saunders, 1971.)
8 What is the Tip-Edge bracket?
The Tip-Edge bracket or appliance developed by P.C. Kesling
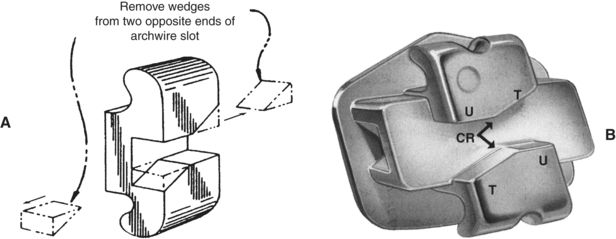
FIG 7-5 A, Removal of diagonally opposed corners of a conventional edgewise bracket arch wire slot to create the basic Tip-Edge bracket. B, The addition of a horizontal tunnel intersects the vertical slot, therefore the bracket profile remains low. The tipping surfaces (T) limit the degree of initial crown tipping, and the uprighting surfaces (U) control final tip and torque angles for a specific tooth. The central ridges (CR) provide vertical control during the noted tooth movements.
(Reprinted from Kesling PC: Tip-Edge Plus Guide, edition 6. La Porte, IN: TP Orthodontics, Inc., 2006. With permission from Dr. Peter C. Kesling.)
9 How did the edgewise appliance evolve?
En masse movement of teeth, particularly in an anteroposterior direction, was extremely difficult with the ribbon arch appliance. Dr. Angle changed the bracket format; he placed the slot in the center of the bracket and fitted the bracket slot in a horizontal plane to the band rather than vertically. One could say that the vertical bracket now had its edge in a sidewise position; arch wire insertion accordingly was with the edge on its side, hence the very appropriate term edgewise appliance.
10 What made the new edgewise bracket different from the original pin and tube vertical bracket?
The vertical bracket had two walls and a pin held the arch wire in place. The new edgewise bracket, 0.022 × 0.028 inch in dimension with the slot opening horizontally, consisted of a rectangular box with three walls within the bracket. The new design provided a more efficient mechanism with which to torque teeth.
11 Who started the first pure edgewise specialty practice?
A student of Dr. Edward Angle, Dr. Charles H. Tweed, followed Dr. Angle’s advice that one could only master the edgewise appliance if the practitioner limited the practice solely to the use of this appliance. Tweed, who received the first specialty certificate in Arizona, devoted 42 years to the advancement of the edgewise appliance. The Tweed philosophy has undergone contemporary changes and is still taught at the Tweed Foundation for Orthodontic Research in Tucson, Arizona, where it has developed the reputation as one of the finest basic edgewise courses.
12 How is the arch wire in the edgewise appliance held in place?
Various methods are used, ranging from the original brass wire ligature to delicate stainless steel wire ligatures; however,elastic o-rings are more often used today (

13 Do all self-ligating brackets function in the same manner during active treatment?
No. Larger twin (Damon
14 What is the difference between full banded versus full direct bonded bracket systems?
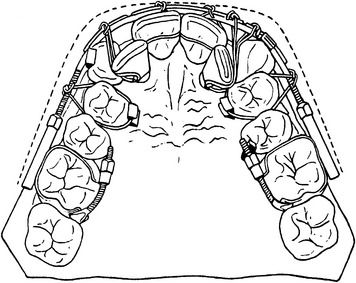
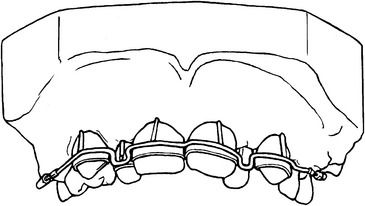
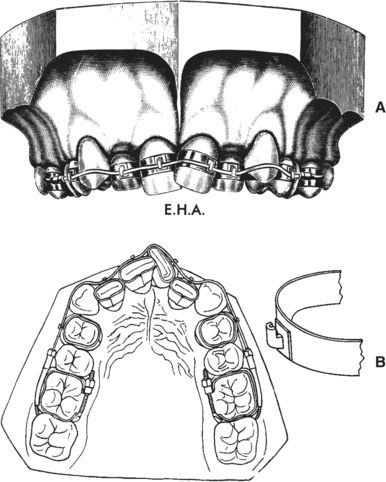
The banded fixed appliance systems use bands cemented to all teeth with various attachments soldered or laser welded to the bands (

15 What is meant by the bracket prescription or preadjusted appliance?
Tooth movement normally occurs in three dimensions. The dimensions were originally incorporated in the edgewise mechanotherapy by specific adjustments to the arch wires, since the first generation of brackets was known as standard edgewise brackets with no prescription. The arch wire adjustments are called first-, second-, and third-order bends. First-order bends are the so-called in-out bends, which are represented by the distance of the bracket slot to the tooth surface and is a horizontal adjustment. This accommodates for the differences in the buccal tooth anatomy. Second-order bends refer to the vertical adjustments, up and down or tip bends, to provide correct axial inclination and tooth-root alignment in a mesiodistal dimension. The mesial to distal tip of the bracket slot in respect to the long axis of the tooth represents this adjustment of the bracket prescription. Third-order or torque adjustments refer to the bucco-palatal or bucco-lingual position of the roots in respect to the crowns of the teeth. All three orders are built into the bracket by the manufacturer and thus represent the prescription of contemporary brackets and in turn meet the requirements of the straight-wire or preadjusted appliance.
16 How does tooth movement occur with fixed appliances?
Tooth movement occurs when a force is applied to the tooth through the bracket, usually an elastic band, coil spring, or specific types of loops or bends in the arch wire. This initiates the resorption of bone on the pressure side and deposition of bone on the tension side of the tooth: the biologic process of tooth movement. A moment is created as a result of the distance of the force application to the center of resistance of the tooth. The center of resistance coincides with the centroid of the root, which in a single-rooted tooth is the geometric center of the root between the apex and alveolar crest. Depending on the significance of the moment, the tooth will translate, tip, or rotate. The latter movements are obviously influenced by the contact of the arch wire and the bracket; thus, a full-thickness arch wire will allow a different type of movement when compared with a thinner dimension and likely more flexible arch wire. In most instances several stages of tooth movement occur with fixed appliances. Examples of these stages include the initial level and alignment stage using smaller size wires, which could be a flexible nitinol or supercable of 0.016-inch s/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


