Periodontal Considerations in the Evaluation and Treatment of Dentofacial Deformities
Teeth
General Information (Fig. 6-1)
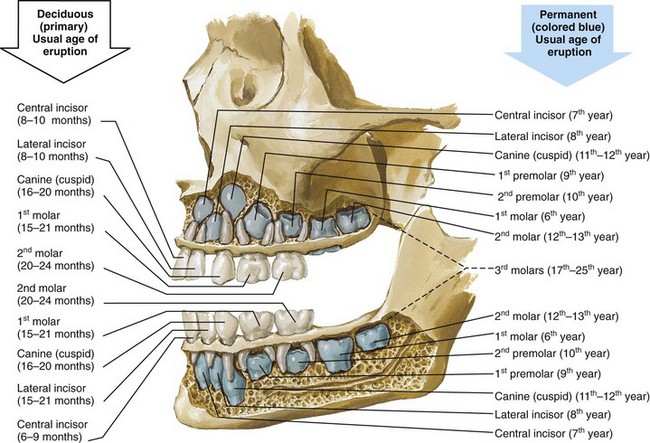
Figure 6-1 Illustration of a sagittal view of a maxilla and mandible with the outer cortex of bone removed to demonstrate a fully erupted deciduous (primary) dentition and the location of the developing permanent tooth buds. Also indicated on the illustration are the usual ages of dental eruption for each tooth of both the deciduous and the permanent dentitions. From www.netterimages.com. © Elsevier Inc. All rights reserved.
Descriptions of the Surfaces of the Teeth (Fig. 6-2)
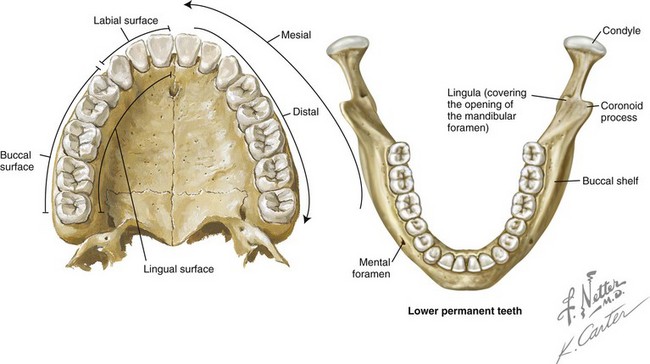
Figure 6-2 Illustrations of the fully erupted permanent dentition in the maxilla and mandible. The palate and the lingual view illustration are used to define terminology for the surfaces of a tooth. From www.netterimages.com. © Elsevier Inc. All rights reserved.
Labial: The surface of the anterior teeth that is closest to the lip
Buccal: The surface of the posterior teeth that is closest to the cheek
Facial: A synonym for labial or buccal
Lingual: Opposite the tongue in the mandibular arch and opposite the hard palate in the maxillary arch
Mesial: Closest to the midline of the dental arch
Distal: Farthest from the midline of the dental arch
Basic Anatomy of a Tooth (Fig. 6-3)
Crown
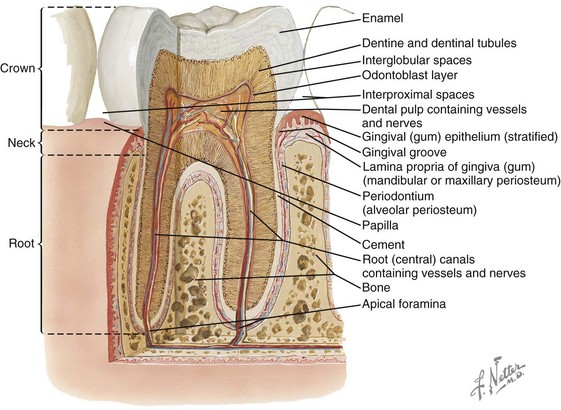
Dentin
• The dentin is the hard tissue that underlies both the enamel and the cementum and that constitutes the major portion of the tooth. Dentin is a modification of osseous tissue. It is composed of a number of dental tubules (small, wavy, and branching tubes) that are located in a dense matrix.
• Dentin is 70% inorganic material by weight, 20% organic material, and 10% water.
The Tissues of the Periodontium
The periodontium includes the investing and supporting tissues of the teeth. It consists of two parts: the attachment apparatus (the cementum, the alveolar bone, and the intervening PDL) and the dentogingival unit (the gingival connective tissue that inserts into the supracrestal cementum and the sulcular and junctional epithelium as well as the latter’s attachment to enamel) (Fig. 6-4). The cementum covers the root surfaces. It serves as the attachment for the fibers of the PDL to the tooth as does the (cortical) alveolar bone of the alveolar socket. The periodontium is affected by the individual’s unique maxillofacial skeletal anatomy, by functional (occlusal) forces, and by degenerative cellular changes that occur with age. The greatest modifier of the periodontium is inflammatory disease.

Figure 6-4 Intraoral view demonstrating the normal width of attached gingiva in the human permanent dentition. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 2-3.
The oral epithelium consists of three zones (Figs. 6-5 and 6-6):
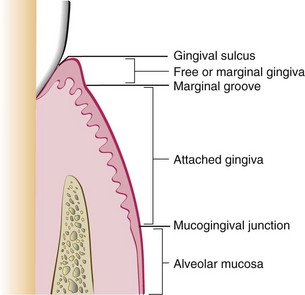
Figure 6-5 Diagram showing the anatomic landmarks of the gingiva. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 2-2.
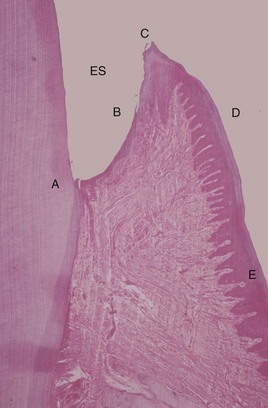
Figure 6-6 Histologic appearance of healthy gingiva. A photomicrograph of a demineralized tooth with the gingival tissues in situ (hematoxylin and eosin stain, low magnification). The amelocemental junction (A) and the enamel space (ES) are shown. Gingival health is characterized by the organization of the epithelium into distinct zones: the junctional epithelium (A to B), the sulcular epithelium (B to C), the free gingiva (C to D), and the attached gingiva (D to E). The gingival connective tissue is composed of densely packed, organized, and interlacing collagen bundles. There are a few scattered inflammatory cells, but there is no significant inflammatory cell infiltrate. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 21-1.
1. Masticatory mucosa (keratinized tissue): This includes the gingiva, the hard palate, and the dorsal surface of the tongue. The gingiva is a fibrous investing tissue that immediately surrounds and is contiguous with its PDL and with the mucosal tissues of the mouth. Keratinized epithelium also covers the hard palate.
• Attached gingiva: This is the portion of the gingiva that is firm, dense, stippled, and tightly bound to the underlying periosteum, tooth, and bone.
• Free gingiva: This part of the gingiva surrounds the tooth and is not directly attached to the tooth surface.
• Marginal gingiva: This is most coronal portion of the gingiva. This term is often used to refer to the free gingiva that forms the wall of the gingival crevice in a normal, healthy mouth.
• Crevicular (sulcular) epithelium: This is the non-keratinized epithelium of the gingival crevice.
• Junctional epithelium: This involves a single layer or multiple layers of non-keratinized cells that adhere to the tooth surface at the base of the gingival crevice. This was formerly called the epithelial attachment.
2. Lining mucosa (non-keratinized tissue): This epithelium makes up the majority of the mucosa of the mouth and is the primary lining of the oral mucosa.
3. Specialized mucosa: This is found specifically in the regions of the taste buds on the dorsum of the tongue.
The gingiva is the part of the oral mucous membrane that covers the occlusal aspect of the alveolar processes of the jaws and that surrounds the necks of the teeth. The junctional epithelium and the connective tissue attachment have a characteristic dimension of 2 to 4 mm; this zone of tissue is called the biologic width. In general, an individual can only maintain health when the sulcus depth is no more than 3 to 4 mm. Greater depth provides a safe haven for bacteria that cannot be easily removed through normal oral hygiene maneuvers. A lower-than-average alveolar crest level is acceptable as long as it is stable (i.e., not progressive) and the periodontium is free of active disease. On the palatal surface of the teeth, the attached gingiva blends with the equally firm and highly keratinized palatal (masticatory) mucosa. The interdental gingiva occupies the gingival embrasure (i.e., the interproximal space beneath the area of tooth contact). It consists of the facial papilla, the lingual papilla, and the valley-like depression that connects the two in the interproximal contact area, which is called the col. In the absence of proximal tooth contact, the gingiva is firmly bound over the interdental bone; it forms a smooth, round surface without a triangular interdental papilla. The connective tissue of the gingiva is densely collagenous, and it contains collagen fiber bundles called gingival fibers (Fig. 6-7). When these fiber bundles insert into the tooth’s cementum, they are called Sharpey’s fibers, and they result in the mechanical attachment of the sulcular and supracrestal (i.e., crestal to the alveolar process) gingiva. These fibers are able to withstand masticatory forces without deflection or detachment from the tooth surface. The connective tissue attachments extend from just apical to the junctional epithelium of the sulcular (crevicular) gingiva to the supracrestal cementum of the root.

Figure 6-7 Diagram of the gingival dental fibers that extend from the cementum (1) to the crest of the gingiva, (2) to the outer surface, and (3) external to the periosteum of the labial plate. Circular fibers (4) are shown in cross-section. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 2-20.
Aging and the Periodontium
The prevalence of periodontal disease with tissue destruction and the loss of teeth and tooth structure tends to increase with age.106,155,160,171 Another consequence of age is reduced tissue elasticity through the degeneration of the elastic fibers. Hormonal changes also occur, and these change the local tissue environment. Traditional thinking is that the degenerative gingival changes associated with aging may include recession, diminished keratinization, reduced stippling, decreased connective tissue cellularity, increased intercellular substances, and reduced oxygen consumption. In the PDL, degenerative aging effects are thought to include a decrease in elastic fibers and a decrease in vascularity and mitotic activity. If these effects occur, the ability of the alveolar bone to withstand occlusal forces is diminished. Frequent changes in tooth structure with age are seen, including occlusal wear with a loss of enamel substance that reduces cusp height and inclination. The degree of attrition is influenced by the masticatory musculature, the consistency of the food eaten, and occlusal factors and habits such as clenching and bruxism. A degree of continued tooth eruption usually occurs as teeth wear. As a result, the clinical crown may become longer, which creates further leverage on the bone with masticatory forces. An opposing factor is the fact that the clinical crowns are simultaneously reduced through attrition, often with an equilibrium or balance being present between the teeth and their bony support. The wear of the teeth along the proximal surfaces may also occur, which results in mesial migration. On average, proximal wear reduces the anteroposterior length of the dental arch by approximately 5 mm by the age of 40 years and by twice that by life’s end. When chronic periodontal disease is added to physiologic degenerative aging, the destructive response of the periodontium is exacerbated. There may be continued gingival recession, attrition, and the reduction of alveolar bone height as a result of a combination of these factors.31
Etiology of Periodontal Disease
Gingivitis and Periodontitis
Inflammation of the gingiva, which is also known as gingivitis, is the most common form of gingival disease (Figs. 6-8 through 6-12).1,19,177,183,216 This occurs as a result of local irritants, such as the toxins released by the microorganisms related to dental plaque and calculus. Foreign bodies (e.g., orthodontic appliances, irregular dental restorations) may also serve as local irritants as well as plaque traps. The inflammation caused by local irritants can result in ulcerative, necrotic, and proliferative changes in the gingival tissues.29,30,34,99,165,170,221 When there is deepening of the gingival sulcus, there can be injury to the supporting periodontal tissues; this may become an irreversible process. With continued inflammation, hyperplastic changes of the gingiva occur, and the crest of the gingival margin extends toward the crown. Inflammation causes a proliferation of and a change in the quality of the sulcus and the junctional epithelium such that their normal protective nature becomes dysfunctional. The sulcus becomes a pocket; ulceration through the epithelial barrier with exposure of the underlying connective tissue to the oral cavity is a frequent occurrence. The organisms and their toxins are then able to access the exposed connective tissue, which undergoes further pathologic changes.93,133,135,154,193 As the process continues, the epithelial junction may separate from the root, and the pocket will migrate downward. The epithelium of the lateral wall of the pocket proliferates with inflammatory tissue, which results in varying degrees of degeneration and necrosis. Intrabony periodontal pockets are said to be present when the base is apical to the level of the alveolar bone. The extension of inflammation from the margin of the gingiva into the supporting periodontal tissues marks the transition from gingivitis to periodontitis.6,40,41,107,117,175,200 The essential problem of periodontal disease is the destruction of alveolar bone with a loss of crestal height and PDL destruction. If periodontal disease is left untreated, it will lead to the loosening and loss of the teeth.

Figure 6-8 Photograph of the maxillary anterior dentoalveolar region. Dehiscence of the labial cortical plate of the canine and fenestration of the labial cortical plate of the first premolar are demonstrated. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 2-60.
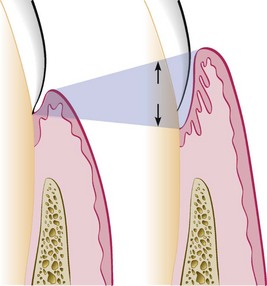
Figure 6-9 Illustration of pocket formation that indicates expansion in two directions (arrows) from the normal gingival sulcus (left) to the periodontal pocket (right). From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 13-1.
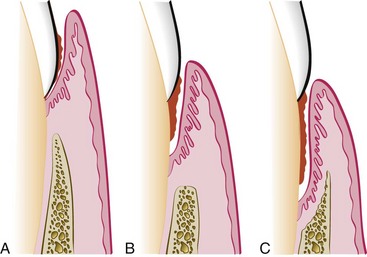
Figure 6-10 Different types of periodontal pockets. With a gingival pocket (A), there is no destruction of the supporting periodontal tissues. With a suprabony pocket (B), the base of the pocket is coronal to the level of the underlying bone, and bone loss is horizontal. With an intrabony pocket (C), the base of the pocket is apical to the level of the adjacent bone, and bone loss is vertical. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 13-2.
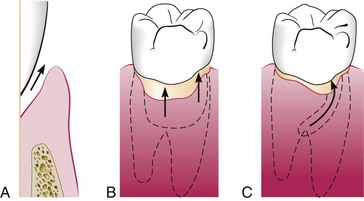
Figure 6-11 Classification of pockets according to involved tooth surfaces. A, Simple pocket. B, Compound pocket. C, Complex pocket. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 13-3.

Figure 6-12 Probing of a deep periodontal pocket. The entire length of the periodontal probe has been inserted into the base of a pocket in the palatal surface of the first premolar. From Newman MG, Takei HH, Klokkevold PR, Carranza FA: Carranza’s clinical periodontology, ed 11, St. Louis, 2012, W.B. Saunders Company, Figure 13-4.
Trauma from Occlusion
Occlusal forces affect the condition and structure of the periodontium.53,54,59,104,129,134,160,181,191,204 To remain structurally and metabolically sound, the PDLs and the alveolar bone require the mechanical stimulation of occlusal forces. When occlusal forces exceed the adaptive capacity of the tissue, injury occurs. The injury that occurs to the periodontium is called trauma from occlusion, and it can be classified as either primary or secondary occlusal trauma. Primary occlusal trauma occurs when greater-than-normal occlusal forces are placed on teeth with a normal periodontal attachment apparatus (i.e., those that are periodontally stable). Secondary occlusal trauma occurs when normal occlusal forces are placed on teeth with compromised periodontal attachment (i.e., those with periodontal disease).
Effects of Orthodontic Appliances and Tooth Movement Forces
Tooth movement during orthodontic therapy is the result of controlled forces placed on the teeth and then transmitted to the PDL. Strong or heavy forces (i.e., forces that far exceed capillary blood pressure) result in the crushing of the PDL on the compression side of the tooth, with local ischemia and degeneration (i.e., hyalinization). Moderate forces that exceed capillary blood pressure result in the compression of the PDL with a delay in bone resorption and the movement of the tooth.89 Light continuous forces that are less than the capillary blood pressure result in only limited ischemia to the PDL, with gradual bone resorption on the compression side.174 The patient’s age is not a contraindication to orthodontic treatment per se. Interestingly, in the adult, the hyalinized (necrotic) zones are formed more readily on the pressure side of the orthodontically moving tooth; this will temporarily slow tooth movement.62 The hyalinized zone is soon eliminated with the reorganization of the tissues, first through the resorption of the marrow spaces (thus undermining resorption) and then through the repair of the PDL and finally of the alveolar bone.172 The anticipated regeneration of the PDL on the compression side and the formation of new bone on the tension side will likely be hampered by the presence of active inflammation in the periodontal tissues (i.e., periodontitis).169 This pathologic response is dependent on how long the PDL remains compromised. This is the reason why inflammation should be controlled through effective periodontal treatment before orthodontic tooth movement.*
Until the mid 1980s, heavy intermittent orthodontic forces were routinely used, and this required patient visits every 3 to 4 weeks.176 This allowed the hyalinized fibers to recover before another heavy orthodontic force was applied. Contemporary orthodontics involves the use of light, continuous force. This moves the teeth with less discomfort and more rapidly, and it also allows visits to be spaced at longer intervals.
In a patient with a periodontally compromised dentition and with a baseline loss of alveolar bone, the center of resistance of the involved teeth moves apically.141,157 The net effect is that the involved teeth are more prone to tipping rather than to bodily movement when orthodontic forces are applied. To achieve improvement in the periodontium, orthodontic treatment requires a combination of light controlled forces as well as the movement of teeth more completely into the alveolar housing. In the presence of active disease, orthodontic therapy should be postponed until effective periodontal treatment is accomplished. This approach to orthodontic tooth movement has been shown to improve any preexisting compromised periodontium.
Teeth that are already tipped outside of the cortical plate (e.g., proclined mandibular incisors in the individual with Class II malocclusion) and that are orthodontically uprighted into sound alveolar housing are likely to improve in overall periodontal health, even when the gingiva levels remain borderline. Animal studies indicate that, without the presence of plaque, orthodontic forces on the teeth do not in themselves induce gingivitis.67 In the presence of plaque, however, similar forces can cause angular bone defects and, with tipping or torquing movements, gingival attachment loss (i.e., recession) can occur.68–70 Clinical studies have demonstrated that, with adequate plaque control, even teeth with longstanding reduced periodontal support can undergo successful tooth movement without further compromise.63 In patients with no active periodontal disease and with good oral hygiene—and even in adults with reduced but healthy residual periodontium—physiologic orthodontic treatment causes no significant detrimental long-term effects on the periodontal attachment, including the bone levels. Physiologic tooth movement involves light forces and the movement of teeth into (not outside of) alveolar bone.37–39
In a cross-sectional study, radiographic crestal bone levels in adults (N = 104) who completed orthodontic treatment at least 10 years previously were shown to be no different than those of matched control subjects (N = 76).161 In a 2-year post orthodontic study, Trosello and colleagues compared adult women who had multi-banded orthodontic therapy (N = 30) with age-matched (non-orthodontically treated) controls (N = 30).203 It was found that the orthodontically treated patients had a higher prevalence of root resorption (17% versus 2%), although there was a lower prevalence of mucogingival defects (5% versus 12%). The root resorption differences were most common in the maxillary incisors, followed by the mandibular incisors. It appears that, in adults, when biologically sound orthodontic maneuvers are carried out, minimal detrimental effects on the health of the periodontium occur. In the short term, gingivitis and gingival hyperplasia may occur, but there is no attachment loss or irreversible effects. In the long term, when the teeth are moved into (not out of) the alveolar bone, mild root resorption (i.e., 1.0 to 1.5 mm) may be documented, but attachment loss (i.e., irreversible change) only occurs in areas of active periodontitis.
It is known that plaque is the primary etiologic factor of gingivitis. A patient’s inability to clean adequately around orthodontic devices (e.g., banded teeth, brackets, wires, springs, coils, elastics, plates) will promote plaque accumulation, which can lead to gingival inflammation. Before the extensive use of bonded brackets, overgrowth of anaerobes in the patient’s sulcus was typical.57 Fortunately, the common practice of placing numerous subgingival orthodontic bands in each quadrant has gone by the wayside. Nevertheless, a shift in the subgingival microflora to a more pathogenic population that is similar to what is seen in periodontal/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


