Flap Classification and Design
Terminology
The primary defect is the wound to be closed by a local cutaneous flap. In this book, the majority of wounds shown have resulted from employing the micrographic (Mohs) surgical techniques to remove skin cancer. A secondary defect is the wound created when a skin flap is transferred to repair the primary defect (Fig. 6-1). The transfer of every cutaneous flap from its in situ position results in a secondary defect. The challenge of reconstructive surgery is to design a flap that places the secondary defect in the most advantageous location. This usually translates into harvesting of the flap from areas of the face and neck that have greater skin laxity.
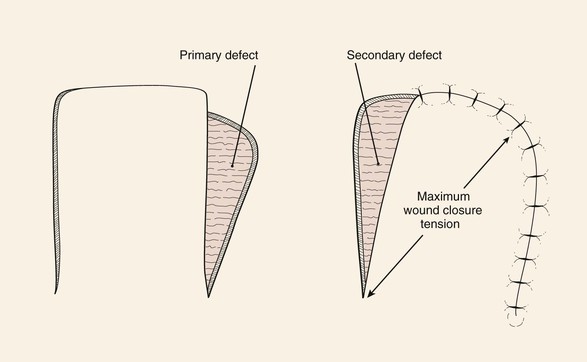
FIGURE 6-1 Movement of cutaneous flap used to repair primary defect creates secondary defect. (From Swanson NA: Classification, definitions, and concepts in flap surgery. In Baker SR, Swanson NA, editors: Local flaps in facial reconstruction, St. Louis, Mosby, 1995.)
When a skin flap is transferred to a defect, the motion of the flap is considered the primary tissue movement of the repair. This usually occurs by sliding or pivoting of tissue. Secondary tissue movement is the displacement of skin surrounding the defect toward the center of the primary defect. The vector of movement is typically in the opposite direction of the vector of movement of the flap. By necessity, there is also skin movement toward the donor site of the flap to close the secondary defect. Therefore, a combination of primary and secondary tissue movement occurs when a wound is repaired with a skin flap (Fig. 6-2). In a region where a primary defect is adjacent to a mobile facial structure, secondary tissue movement may result in distortion of these structures. Facial structures that have visible margins, such as the eyelids, lips, and nostrils, are particularly susceptible to distortion by secondary tissue movement. The stronger the attachments of facial structures to the underlying bone, the less propensity for distortion. For example, the earlobe is more likely to be deformed by secondary tissue movement than the tragus is.
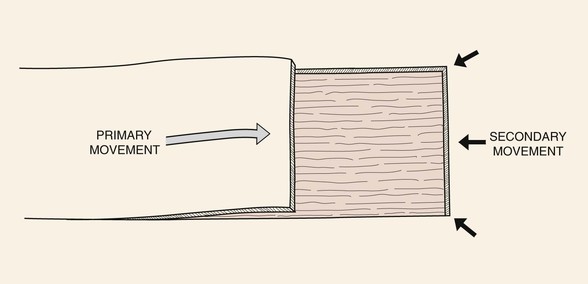
FIGURE 6-2 Combination of primary and secondary tissue movement occurs when a wound is repaired with a skin flap.
In part, the degree of wound closure tension is related to skin extensibility. Skin extensibility is the lengthening of skin under tension due to stretching of elastic fibers. There are directional variations in skin extensibility.1 That is, skin is more extensible when the vector of strain is in a certain direction. For this reason, it is advantageous to recruit skin for repair of a wound in areas of maximum skin extensibility. These areas are identified by the lines of maximum extensibility (LME).
Relaxed skin tension lines (RSTLs) are intrinsic to facial skin. RSTLs result from orientation of collagen fibers of the skin and are manifested in the aging face as skin creases and wrinkles (Fig. 6-3). RSTLs are perpendicular to LME. The orientation of skin excisions and repair of wounds are usually made parallel to RSTLs when possible (Fig. 6-4). Orienting them this way places the maximum wound closure tension parallel to LME and perpendicular to RSTLs. This orientation results in wound repair that is performed with the least amount of wound closure tension. Minimal wound closure tension is extremely beneficial in minimizing the appearance of facial scars. A converse of this is that incisions made at right angles to RSTLs usually heal with wider and more visible scars.
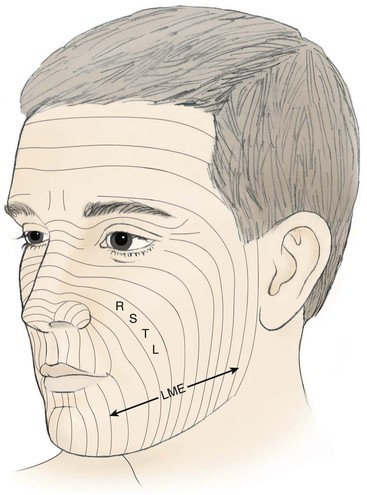
FIGURE 6-3 Relaxed skin tension lines (RSTLs) of face. Lines of maximal extensibility (LME) are perpendicular to RSTLs.
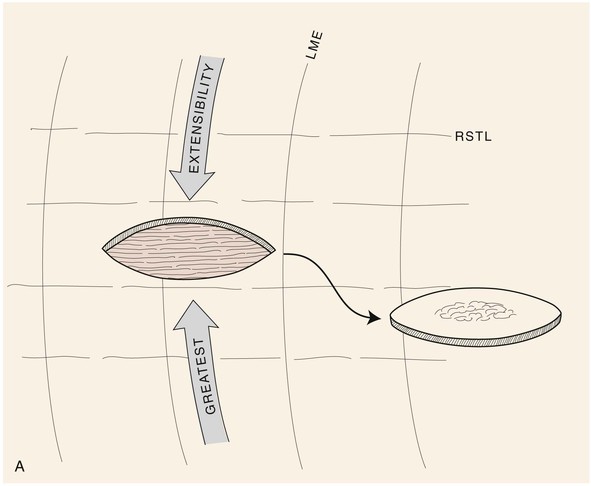
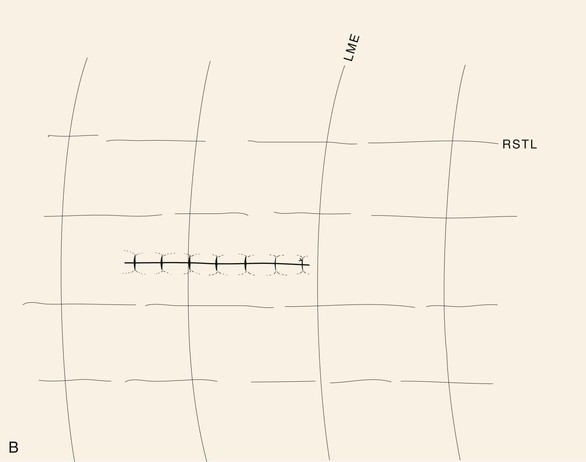
FIGURE 6-4 A, B, Orientation of skin excisions and repair of wounds are made parallel to RSTLs when possible.
An important factor that may limit skin expansion is the attachments of the skin to underlying structures, such as fascial or aponeurotic connections to the skin. Skin expansion is resisted by structures that anchor the skin by aponeurotic or tendinous insertions in bone. Examples of these include medial and lateral canthus, bony orbital rim, zygomatic arch, and malar eminence. Undermining of the skin reduces wound closure tension and more widely distributes skin deformation. Undermining releases the attachments of the skin to the underlying fascia, allowing the skin to become more expansible. Moderate skin undermining is beneficial in reducing wound closure tension. However, extensive skin undermining is not usually helpful in further reducing the wound tension, although it may assist with tissue draping and reduction in secondary tissue movement.
Flap delay is a means of increasing the blood flow to a flap. Delay is accomplished by incising all or a portion of the flap and elevating all or a portion before returning the flap to its in situ position. The incisions are sutured, and the flap is left in place usually for 10 to 14 days before the flap is transferred to a recipient site. Delay results in an enhanced circulation to the flap, probably by the closing of arteriovenous shunts and the realignment of the vasculature in the subdermal plexus. Delay is rarely used with local flaps of the face because of the overall rich blood supply to facial skin. Delay is reserved for particularly large flaps used to repair major facial defects in situations in which skin vascularity has been compromised by irradiation or previous surgery and, on occasion, in patients using tobacco.
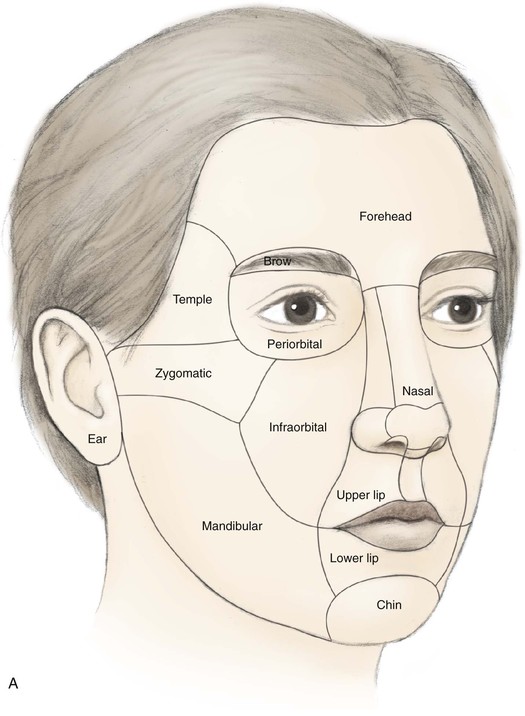
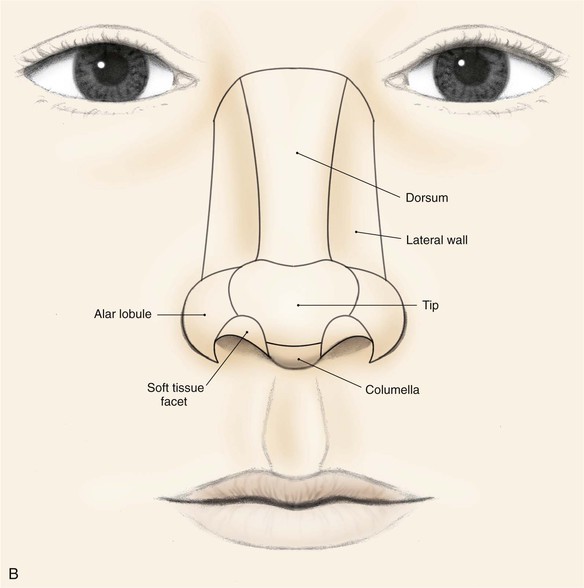
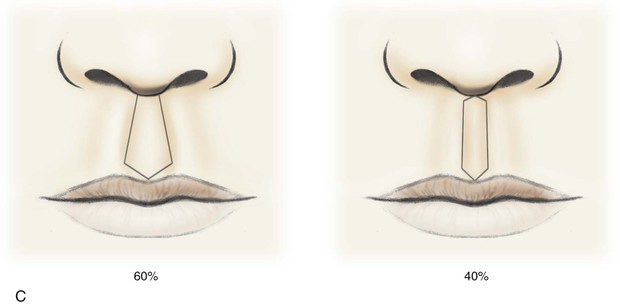
The face can be divided into specific areas or aesthetic regions, which are covered by skin that has common characteristics. These skin characteristics include thickness, quantity of subcutaneous fat, degree of adherence to underlying fascia, color, texture, and hair growth. Coincidentally, these facial areas are separated from each other by ridges or valleys in the skin created by the facial skeleton or musculature. These ridges and valleys are known as aesthetic borders and are identified by facial landmarks including eyebrows, melolabial creases, mental crease, philtral crests, vermilion borders, and anterior hairline. Aesthetic regions and their accompanying borders provide form, character, and individual uniqueness to the face. The principal aesthetic regions of the face are forehead, eyelids, cheeks, nose, lips, mentum, and auricles (Fig. 6-5). Some aesthetic regions may be divided into a number of components known as aesthetic units, which are separated by borders somewhat less discrete than those that delineate aesthetic regions. The forehead may be divided into central and temporal units. The cheek is divided into infraorbital, zygomatic, buccal, and parotid masseteric units. The upper lip is divided into philtrum and paired lateral units. The lower third of the face is divided into labial and mental units. The nose is particularly suited for division into aesthetic units because of its complex topography. It may be divided into nine aesthetic units that include dorsum, paired sidewalls, tip lobule, paired nasal facets, paired alae, and columella. These units are highlighted when incident light is cast on the nasal surface, creating shadows along the borders of each unit and topographic landmarks.2 As with facial aesthetic units, the framework of the nose supporting the overlying skin is primarily responsible for variations in light reflections and gives rise to the aesthetic border between the nasal units.
Local Flap Classification
Cutaneous flaps may be classified by the nature of their blood supply (random vs. arterial), by configuration (rhomboid, bilobe), by location (forehead, cheek, lip), and by the method of transferring the flap. Flaps classified by location are identified by the region of the body from which they are harvested. This location may be near or considerably removed from the primary defect. When they are removed from the defect, such flaps are transferred either by microvascular surgery or by staged movement of the flap toward the recipient site. On the basis of location, flaps are classified as local, regional, or distant. A local flap is one in which tissue immediately adjacent to or near the primary defect is used to cover the defect. The majority of skin flaps discussed in this textbook are local flaps. In regard to facial reconstruction, a regional flap is one in which tissue is harvested from a site not located on the face, scalp, or neck. However, the pedicle is sufficiently long to enable the flap to reach the primary defect. An example of a regional flap for facial repair is a deltopectoral flap transferred from the anterior chest wall to repair a defect of the lip or cheek. A distant flap is one that is harvested from sites so removed from the face that the pedicle is not sufficiently long to enable the flap to reach the face. Distant flaps are usually transferred to the face as free flaps, sometime referred to as microsurgical flaps. The blood vessels of their pedicle are connected to vessels in the head or neck by microvascular surgical techniques. Another way of transferring distant flaps to the face is by staging tubed flaps, in which the pedicle is “walked” toward the recipient site. This method has been abandoned since the development of microsurgical techniques.
The most common way to classify flaps on the basis of blood supply is to categorize them as random or axial pattern flaps. This is discussed in detail in Chapter 2. Random pattern flaps are based on the rich perforating vascular plexus of the skin (Fig. 6-6). They do not have a named blood vessel providing vascularity to the flap. In contrast, axial pattern flaps depend on a named artery for the majority of their blood supply (Fig. 6-7). These vessels parallel the linear axis of the flap and are usually located in the subcutaneous fat directly beneath the skin of the flap. Most axial pattern flaps have a degree of random pattern vascularity to their distal portion. The majority of cutaneous flaps of the face are random pattern. The most common axial pattern flap harvested from the face is the paramedian forehead flap based on the supratrochlear artery and vein.
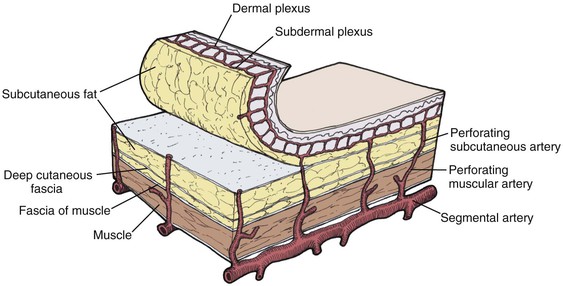
FIGURE 6-6 Random pattern flaps based on subcutaneous and intradermal vascular plexuses that supply blood to skin. (From Swanson NA: Classification, definitions, and concepts in flap surgery. In Baker SR, Swanson NA, editors: Local flaps in facial reconstruction, St. Louis, Mosby, 1995.)
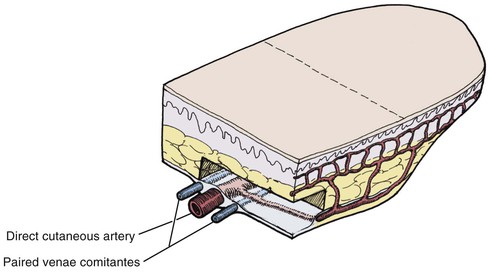
FIGURE 6-7 Axial pattern flaps based on named artery for blood supply. Most axial pattern flaps have a degree of random pattern to the distal portion. (From Swanson NA: Classification, definitions, and concepts in flap surgery. In Baker SR, Swanson NA, editors: Local flaps in facial reconstruction, St. Louis, Mosby, 1995.)
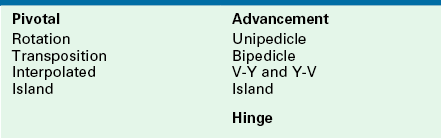
Classifying flaps by method of transfer, which is to say method of tissue movement, is usually the most convenient way of discussing flaps relative to their use in repair of facial cutaneous defects (Table 6-1).3–5 This classification divides local flaps into pivotal, advancement, and hinge. Advancement in the majority of situations depends on stretching the flap skin in the direction of flap movement. Such flaps are subjected to an increase in wound closure tension. In contrast, pivotal flaps rotate about a point at their base and in their purest form are not stretched. Thus they are not subjected to wound closure tension greater than the natural tension of the remaining facial skin, although the repair of the donor site of the flap is subjected to increased skin tension. However, in most circumstances in which pivotal flaps are used, tissue movement is achieved through a combination of pivoting and advancement. That is, movement of most pivotal flaps is aided by stretching (advancement) of the flap skin. Surgeons often speak of combined mechanisms of tissue movement, such as “advancement rotation flap.” For clarity, the major mechanism of tissue movement should dictate the term given to describe a particular flap, unless both mechanisms are of approximately equal importance.
Pivotal Flaps
There are four types of pivotal flaps: rotation, transposition, interpolated, and island. All pivotal flaps are moved toward the defect by pivoting the flap around a fixed point at the base of the pedicle. Except for island flaps skeletonized to the level of their nutrient vessels, the greater the pivot, the shorter is the effective length of the flap (Fig. 6-8). Pivoting a flap with a cutaneous pedicle 45° from its in situ position reduces the effective length 5%. A 90° and 180° pivot reduces effective length by 15% and 40%, respectively.6 The reduction in effective length must be accounted for when pivotal flaps are designed so that greater pivoting requires a longer design of the flap. As the flap turns in an arc around its relatively fixed pivotal point, redundant tissue, known as a standing cutaneous deformity (dog ear), develops at the base. Similar to effective length, there is a positive correlation between the degree of pivoting and the size of the standing cutaneous deformity. The greater the pivot of the flap, the larger the deformity that occurs. Thus, increasing the flap’s pivot will change the flap’s shape, shorten the effective length, increase wound closure tension, and deform the flap’s base by development of a standing cutaneous deformity. To limit these restricting factors, a flap’s arc of pivot should not exceed 90° whenever possible.
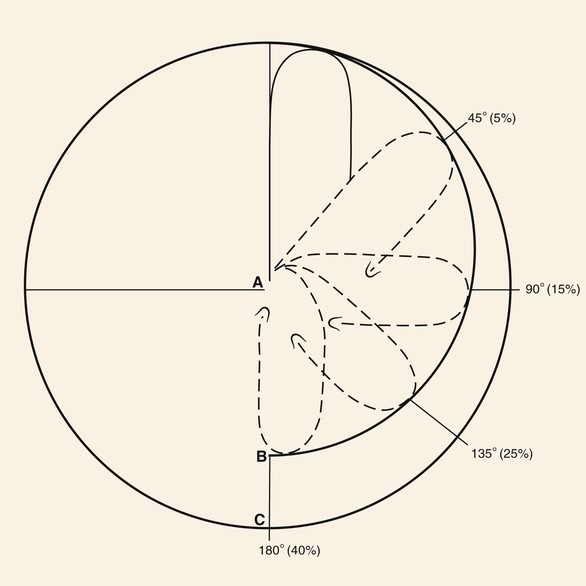
FIGURE 6-8 As transposition flap pivots, flap changes shape and shortens as standing cutaneous deformity increases. As flap pivots about point A, effective length of flap decreases along circumference B rather than C. Approximate percentage of shortening as related to degree of pivotal movement is in parentheses. (From Panje WR, Minor LB: Reconstruction of the scalp. In Baker SR, Swanson NA, editors: Local flaps in facial reconstruction, St. Louis, Mosby, 1995.)
Rotation Flaps
Rotation flaps are pivotal flaps with a curvilinear configuration. They are designed immediately adjacent to the defect and are best used to close triangular defects. In such instances, the triangle-shaped defect is covered by a portion of the standing cutaneous deformity, thus facilitating the pivotal movement of the flap (Fig. 6-9). This flap usually makes use of some advancement, and when it does, the vector of greatest wound closure tension is along a line from the base of the flap to a distal point of the curvilinear border. When no advancement is used in movement of the flap, animal studies have shown the greatest wound closure tension to be at the closure site perpendicular to the periphery of the flap, not across the long length of the flap.1 These studies have also demonstrated minimal mechanical benefit at the defect site in extending the arc of rotation flaps beyond 90° from the axis of the primary defect. However, there may be benefit in extending the incision to accommodate redraping of skin. A back cut at the base of the flap shifts the position of the pivotal point and thus changes the wound closure tension vector as well as the location of the standing cutaneous deformity.
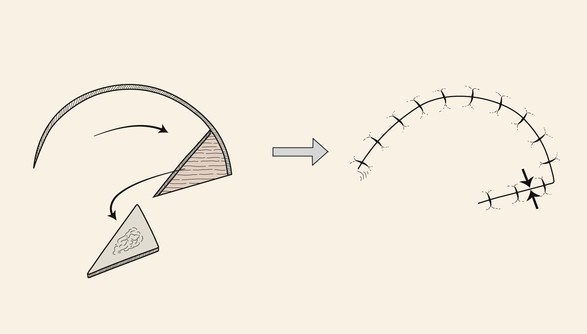
FIGURE 6-9 Rotation flaps are pivotal flaps with curvilinear configuration. They are designed immediately adjacent to defect and are best used to repair triangular defects. Opposing arrows indicate greatest wound closure tension.
Disadvantages of rotation flaps are relatively few. The defect itself must be somewhat triangular or must be modified by removal of normal tissue to create a triangular defect. The configuration of the flap includes a right angle at the distal tip, and the surgeon must take care in positioning the tip so that it is not subjected to excessive wound closure tension and vascular compromise. The curvilinear incision necessary to create the flap does not easily lie in RSTLs (see Fig. 6-3). As with all pivotal flaps, rotation flaps develop standing cutaneous deformities at their base that may not be removed without compromising vascularity. A second-stage revision in which the standing cutaneous deformity is removed may be necessary.
Transposition Flaps
In contrast to rotation flaps, which have a curvilinear configuration, transposition flaps have a linear configuration. Both are pivotal flaps moving about a pivotal point. Both flaps develop standing cutaneous deformities at their bases, and as a consequence, their effective length decreases as they pivot. This reduction in effective length must be considered in designing such flaps. Rotation flaps must be designed in such a way that one border of the flap is also a border of the defect for which it is intended for repair. Like rotation flaps, transposition flaps may be designed so that one border of the flap is also a border of the defect (see Fig. 6-1); however, it may also be designed with borders that are removed from the defect (Fig. 6-10). In this circumstance, only the base of the flap is contiguous with the defect. The area of greatest wound closure tension is at the closure site of the secondary defect adjacent to the base of the flap. Depending on whether the flap is stretched and the degree of stretching, the greatest wound closure tension may be along a vector from the pivotal point to the most peripheral border of the flap. The ability to construct a flap some distance from the defect with its axis independent from the linear axis of the defect is one of the greatest advantages of transposition flaps. This fact enables the surgeon to recruit skin at variable distances from the defect, selecting donor sites with the greatest skin elasticity or redundancy. In addition, the ability to select a variable site for harvest of a flap may allow the selection of a donor site that will provide the best possible scar camouflage or even the ability to hide the scar in aesthetic boundaries.
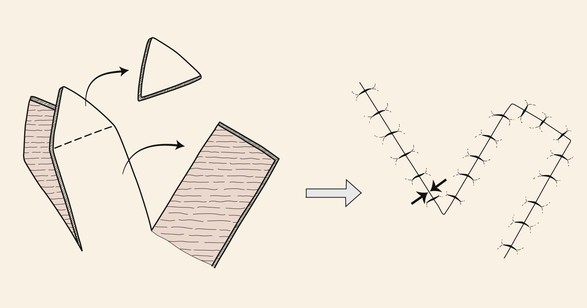
FIGURE 6-10 Transposition flaps are pivotal flaps with linear axes. The base of the flap is contiguous with the defect. Greatest wound closure tension is at closure site of donor defect (opposing arrows).
Transposition is the most common method of transferring local flaps to skin defects of the head and neck. A transposition flap is a reconstructive option for small to medium-sized defects of almost any conceivable configuration or location, thus making it the most useful of local flaps in facial reconstruction (Fig. 6-11).





FIGURE 6-11 A-E, Transposition flaps are common reconstructive options for small to medium-sized cutaneous cheek defects. A, Lentigo maligna outlined by sutures. Transposition flap designed. B, Skin lesion excised, standing cutaneous deformity (SCD) marked for excision at base of flap. C, Flap in place. D, E, At 1 year after surgery. No revision surgery performed.
Two types of transposition flaps frequently used are rhombic flaps and bilobe flaps. Rhombic flaps depend on advancement for part of their tissue movement, but the majority of movement is pivotal. A rhombus is an equilateral parallelogram. A rhombus defect may be thought of as two equilateral triangles placed base to base to form a rhombus with adjacent angles of 60° and 120°. All sides and the short diagonal of the defect must be equal in length in a 60°–120° rhombus defect and flap (Fig. 6-12). Once the 60°–120° rhombus defect has been created with all sides equal in length, the flap is designed by directly extending the short diagonal a distance equal to all other sides. This creates the first side of the flap. The second side of the flap, again equal in length to all other sides, is drawn parallel to one of the adjacent borders of the defect.7
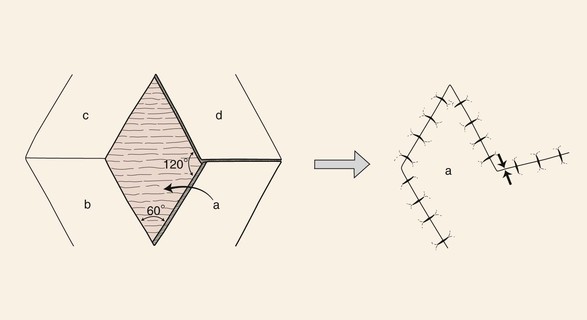
FIGURE 6-12 For every rhombus defect, four potential flaps may be designed. Greatest wound closure tension is at donor site (opposing arrows).
The greatest wound closure tension with a rhombus flap is at the donor site and has been calculated to be 20° from the short diagonal line across the base of the flap.7 Wide undermining of the surrounding tissue has minimal effect on the wound closure tension. Thus, in designing the flap, skin mobility and extensibility are important. Understanding the vector of the resultant wound closure tension is critical to avoid distortion of surrounding structures. For every rhombus defect, four potential flaps may be designed (Fig. 6-12). The surgeon can quickly visualize the resulting scar configuration and approximate vector of maximum wound closure tension by drawing the flap and then covering the two parallel sides of the flap with his or her fingers.
The design of the rhombus flap is more complex than that of most other facial skin flaps because of the geometry and option of placing the flap in four separate locations about a rhombus defect. The author does not use the rhombus flap or its variations frequently, primarily because approximately half of the entire length of the scar that results from use of the flap is not parallel or does not lie within RSTLs. This disadvantage is most important in the area of the forehead, where skin creases are more prominent. RSTLs are less important in the cheek, where creases are not as prominent, the skin is thinner, and the resulting scar from the use of a rhombus flap tends to blend better with adjacent skin.
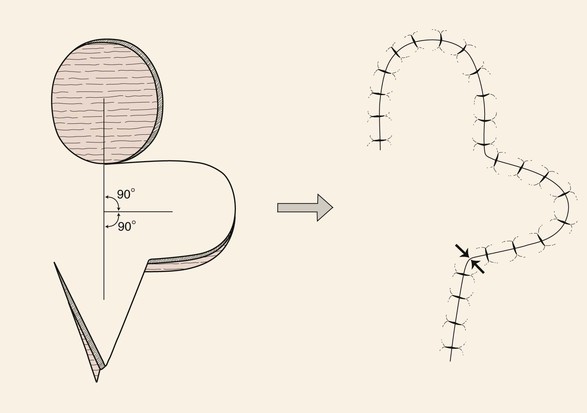
The bilobe flap is a double transposition flap that shares a single base. Each lobe of the flap has a separate pivotal point, and thus each has a standing cutaneous deformity.8 It was originally designed for repair of nasal defects but has frequently been used to reconstruct cheek defects as well. In the classic design of the bilobe flap, the axes of the first and second lobes as well as the defect were all separated by an angle of 90° (180° total) (Fig. 6-13). This design transferred the tension of the wound closure through a 90° arc, which is more than the usual 45° to 60° arc of a single transposition flap. This greater movement about a pivotal point, together with the use of two tissue flaps, assists in minimizing wound closure tension of the primary and secondary defects.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


