45 Endodontics in the Deciduous Dentition
Endodontic treatment of deciduous teeth is quite different from that of the mixed dentition or permanent teeth. This is due to the quite different morphologic/anatomic peculiarities of the deciduous teeth, and also often due to limited cooperation by the child patient. For example, 50%–70% of children under 5 years of age have untreated primary tooth caries, and within this group, 20% already exhibit the need for comprehensive dental treatment.
The high level of untreated and often progressive caries in primary teeth correlates with the high endodontic treatment needs of child patients. This is also directly due to specific anatomic characteristics of these teeth. Rapid progression of dental caries and early pulpal involvement in the deciduous dentition require a special treatment concept. The scenario is highly problematic in that it requires consideration of the psychologic components in addition to the pure dental findings and the stage of development of the entire dentition.
For this reason, the comprehensive treatment of the deciduous dentition necessitates giving a higher level of priority to the prevention of pain and infection, any space loss in the arches, and any other damage to the permanent dentition.
45.1 Deciduous tooth morphology
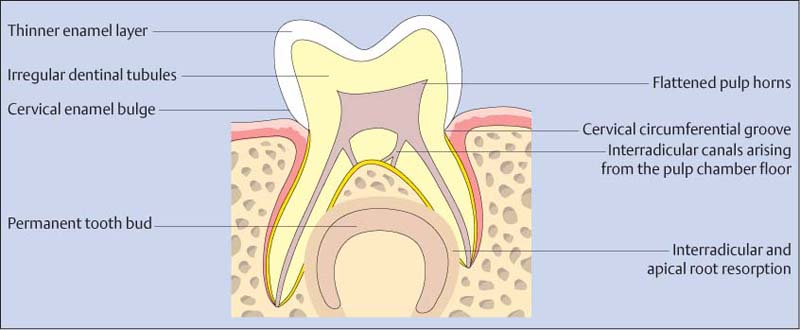
In comparison with the permanent dentition, the pulp of deciduous teeth relative to the tooth crown is larger. The thinner enamel layer, as well as the micromorphologic characteristics of the dentin, favors rapid spread of caries. In comparison with the tooth crown, the root is longer. The proximal contacts in the molar area are broad.
45.2 Value of the deciduous molars
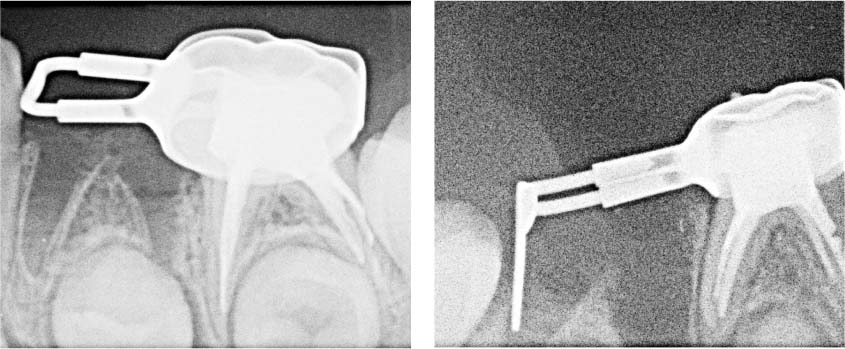
Left: Importance of the second deciduous molar following loss of the first deciduous molar, for anchoring a space maintainer. Note that the permanent first molar is in the process of erupting.
Right: Root canal filling of the first deciduous molar for anchoring a so-called distal-shoe space maintainer following loss of the second deciduous molar.
45.3 Significance of the canines
Left: The primary canine has been described as the “pillar” of the deciduous dentition: It prevents mesial drifting of the molars.
Right: The strategically important canines and second molars should be retained whenever possible.
Goals and Diagnosis
Deciduous teeth play an important role in the growing child. In young children, maintenance of the anterior teeth is critical for speech development, especially learning sibilant sounds, as well as preventing the development of improper tongue function. Even in older children, molars, depending on the stage of development of the permanent teeth, are important as space maintainers for the permanent teeth. Additional goals include the maintenance of masticatory function, freedom from pain, and prevention of infections, as well as secondary damage to the permanent dentition. Direct evaluation of pain is particularly difficult with young children. Frequently, parents will report a child having sleepless nights or loss of appetite, which could be related to endodontic problems. Diagnosis of the problem in the responsible tooth is rendered more difficult because provocation of pain during vitality testing or percussion may lead to lack of cooperation by the child.
Tooth mobility tests, on the other hand, are useful and should be carried out in comparison of the contralateral tooth to exclude normal mobility before exfoliation. It is also helpful to carefully probe the furcation using a curved probe because the special anatomic characteristics (interradicular canals) can lead to tissue destruction in this area, which is a sign of infection.

45.4 Space deficiency
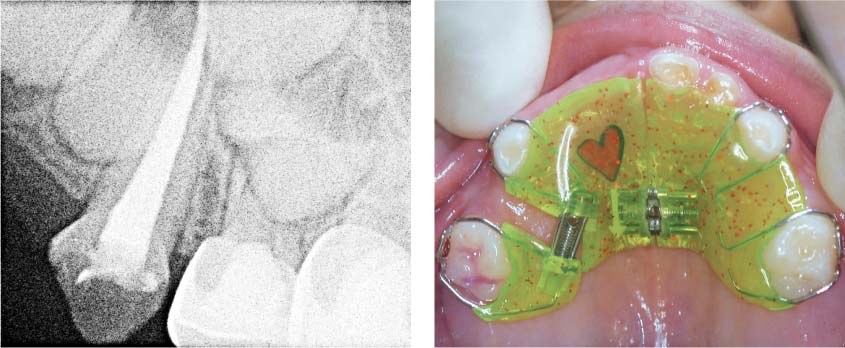
Left: Massive space loss occurred with subsequent crowding because of early loss of the first primary molar.
Right: Severely reduced masticatory function resulting from multiple primary tooth extractions can also have a negative influence on the child’s nutrition. The esthetics are impaired, which could lead to psychological effects. The development of para-functional oral habits is promoted.

45.5 Infections and possible consequences
Left: Buccal abscesses frequently resemble periodontal abscesses. The reason for this is infection in the accessory canals at the floor of the pulp chamber, which cause inflammation in the interradicular area. Note the mesial drift of the molar.
Right: So-called “Turner tooth” (tooth 24). Enamel defect as a result of chronic infection of the deciduous predecessor.

45.6 Clinical diagnosis
Left: The most important diagnostic criterion is the intensity of hemorrhage after opening the pulp chamber. This provides clues as to the extent of the inflammatory process. (Compare with the simultaneous access cavity preparation of teeth 84 and 85. Regarding therapeutic con sequences, see “Summary and Conclusions” on p. 360.)
Right: An infection can spread into the furcation area via the interradicular canals. Following local anesthesia the furcation should therefore be carefully probed.
Radiographic Diagnosis
Between the ages of 4 and 4.5 years, the proximal surfaces of the deciduous molars come into contact, closing the usual moderate spaces between these teeth and thus increasing the likelihood of proximal caries development. If the child is cooperative, a radiographic diagnosis should be made, as the extent of caries is often clinically underestimated.
Radiographs also provide valuable clues to root anatomy, the progression of physiological root resorption already under way, the position of the permanent tooth buds, and possible pathologic alterations.
In contrast to the permanent dentition, infection-elicited osteolysis of deciduous molars usually occurs first in the furcation region due to the accessory canals on the floor of the pulp chamber. Differential diagnosis with regard to purely physiologic root resorption processes is not always simple, so additional clinical probing of the furcation using a curved (Nabors) probe is recommended.
As intraoral radiographs are sometimes not possible due to poor cooperation, or because of parental rejection of radiation exposure, alternative methods may be used, such as the cold light probe or laser assessments. Even with poor cooperation, children tolerate these examination methods better than intraoral radiographs.
45.7 Radiographic diagnosis
Left: Congenitally missing permanent second premolar. Dependent on the stage of development of the first permanent molar and other relative orthodontic considerations, the retention of the second deciduous molar is recommended.
Right: Anatomic variations such as three roots on a primary mandibular molar are a common occurrence in the deciduous dentition.

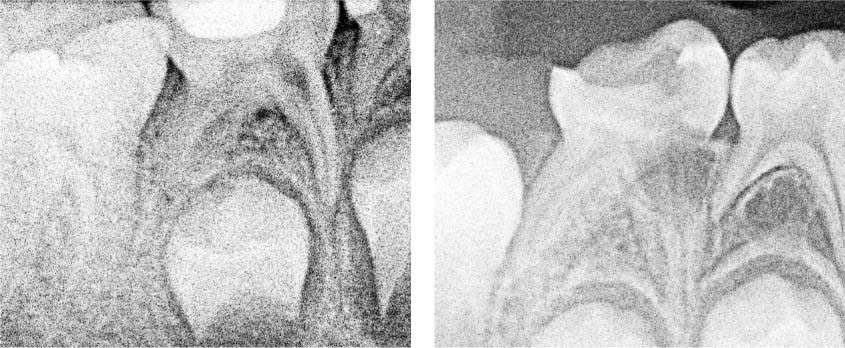
45.8 Radiographic diagnosis
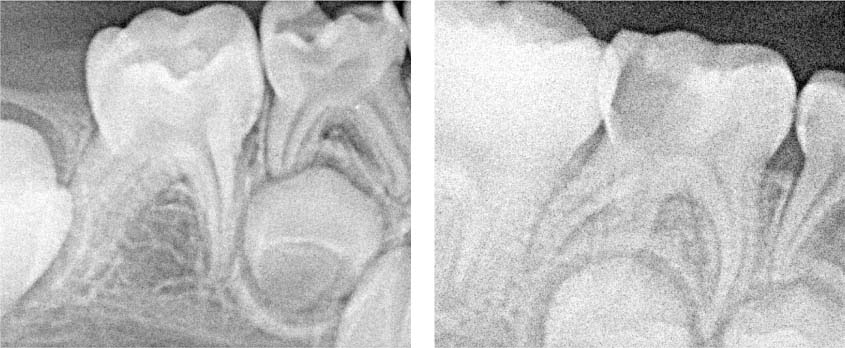
Left: Typical interradicular radiolucency caused by infection from accessory canals on the floor of the pulp chamber.
Right: Periapical radiolucencies are quite rare and usually occur in cases with advanced stages of carious destruction of the crown.
45.9 Radiographic diagnosis
Left: Internal resorption is related to inflammation: Note the restoration near the pulp on tooth 85.
Right: External resorption is also related to inflammation.
Prerequisites for Pediatric Dental Treatment
In addition to proper technique and diagnosis, endodontic procedures in the deciduous dentition depend above all on the child’s level of cooperation. As cooperation is often impeded by acute pain, early treatment of deciduous tooth caries is especially important.
Children can gradually be introduced to treatment with the help of the “tell–show–do” technique. If acute pain and swelling with a tendency to spread are already present, the dentist may also consider prescribing antibiotics to protect the permanent tooth bud.
With very young children who remain noncompliant but are in pain, behavioral management alone may often be unsuccessful without medicinal support. In cooperation with an anesthetic team with pediatric experience, comprehensive dental treatment can be carried out under conscious sedation or, ultimately, general anesthesia.
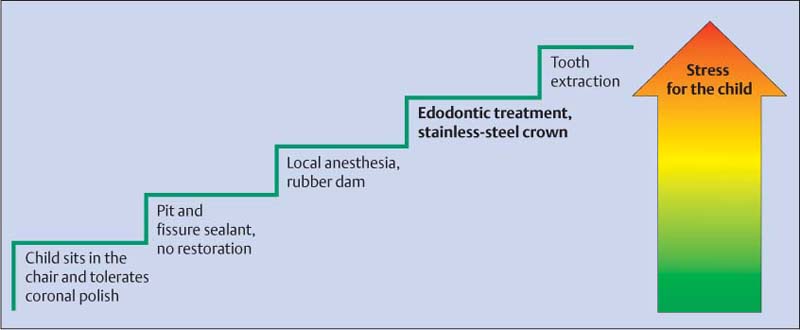
45.10 Behavioral management
“Tell-show-do”: First the ins/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


