CHAPTER 4
Supraperiosteal Transport Distraction Osteogenesis
The second step in the right direction is the most difficult.
—Theo Mestrum
Distraction osteogenesis (DO) is a widely used technique for reconstructing bony defects in the maxillofacial region. This technique provides new bone formation without grafting procedures, but because periosteal reflection may leave a lateral concavity, the new bone sometimes grows with an hourglass deformity. 1 Maintenance of adequate blood supply to transport segments via intramedullary and periosteal routes is critical for producing sufficient bone formation in a distraction gap.2,3 Indeed, medullary continuity may be maintained with corticotomy,2–4 but that procedure cannot always be performed in this region. In contrast, periosteal attachment and continuity can be planned by the surgeon. This chapter presents an osteoperiosteal transport method for DO that minimizes disturbances of the periosteal blood supply to transport segments by using supraperiosteal application of distraction devices.
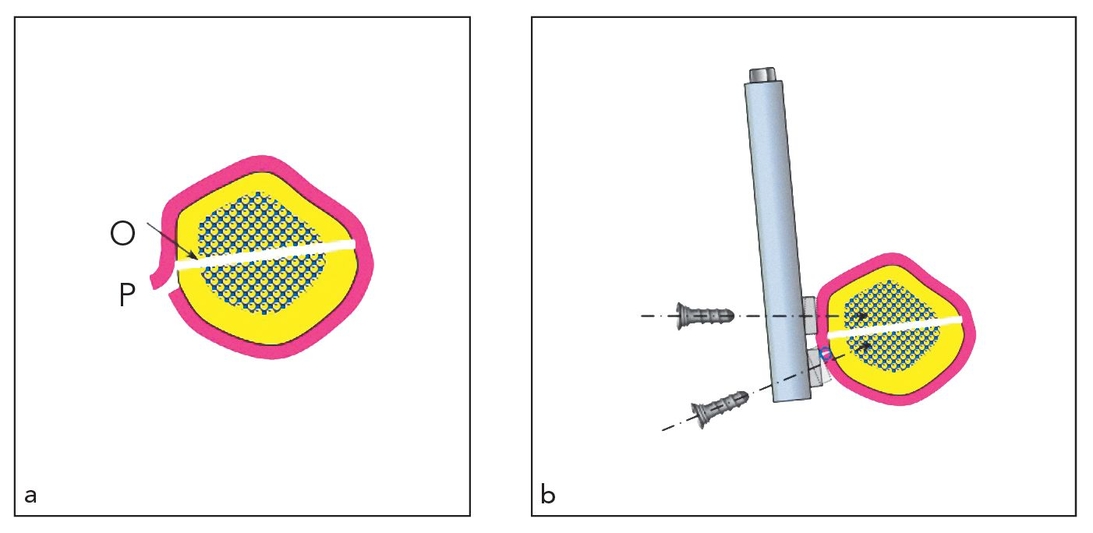
Fig 4-1 (a) A minimal periosteal incision is made 1 to 2 mm away from a planned osteotomy (O) line to create a transport segment. The periosteum (P) is then reflected beyond the line. Following the osteotomy, the periosteum is repositioned and sutured. (b) When a distraction device is fixed supraperiosteally, special care should be taken not to compress the underlying periosteum with plates, and fixation screws should not be fully tightened unless they contain a locking mechanism involving the plates.
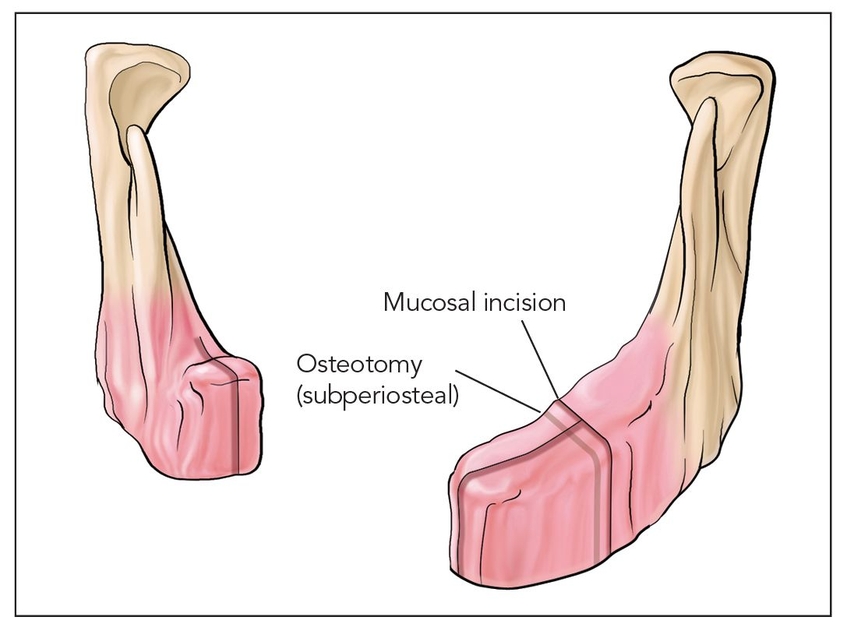
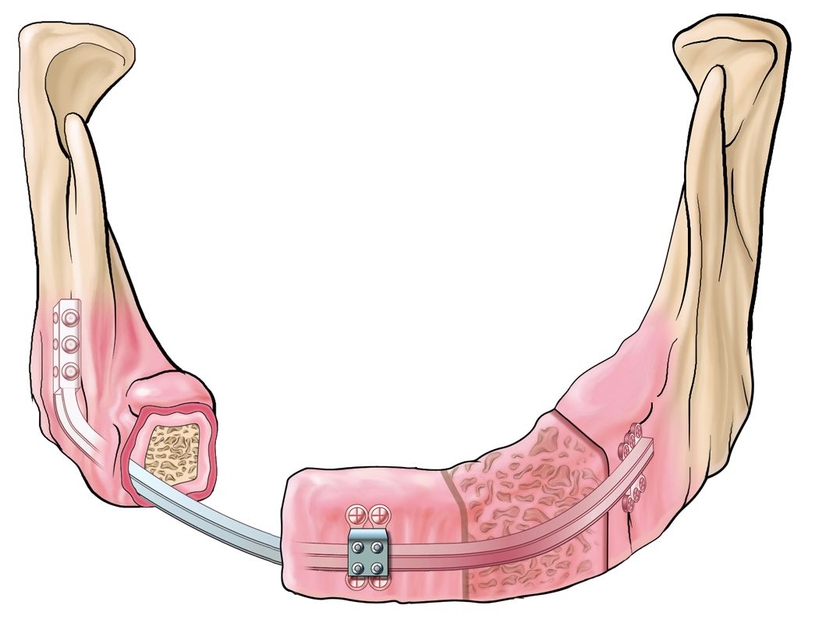
Fig 4-2a A large continuity defect can be treated by supraperiosteal transport DO.
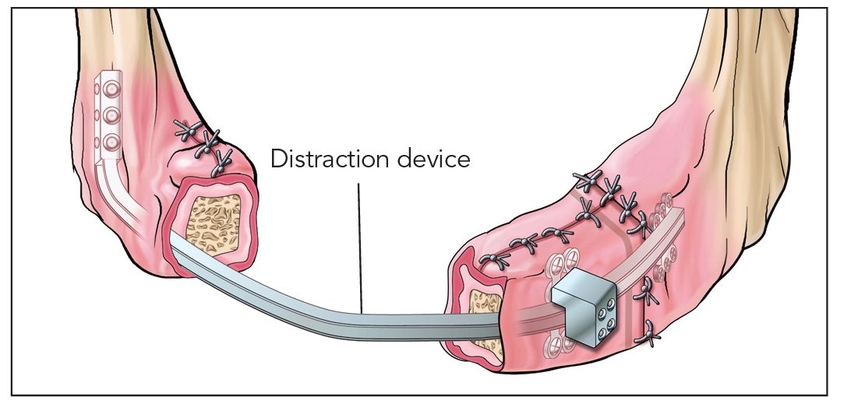
Fig 4-2b The device must be fixed supraperiosteally, taking special care not to compress underlying periosteum with the plates by not fully tightening the fixation screws.
 Surgical Technique
Surgical Technique
A mucosal incision and subsequent supraperiosteal dissection are made to provide an area for seating of the distraction device. A minimal periosteal incision is made 1 to 2 mm away from a planned osteotomy line to create a transport segment, and the periosteum is then reflected beyond this line (Fig 4-1). Following the osteotomy, the periosteum is repositioned and sutured.
In the treatment of a large continuity defect (Fig 4-2a), for example, a distraction device is fixed supraperiosteally (Fig 4-2b). Special care should be taken not to compress the underlying periosteum with the plates, and fixation screws should therefore not be fully tightened unless they contain a locking mechanism with the plates. The wound is closed in layers. The transport segment should move within the limits of periosteal tension according to activation of the distraction device (Fig 4-2c) done over a period of weeks until the transport is “docked” (Fig 4-2d). Six months of healing or more is required before device removal (Fig 4-2e) and subsequent implant placement (Fig 4-2f).
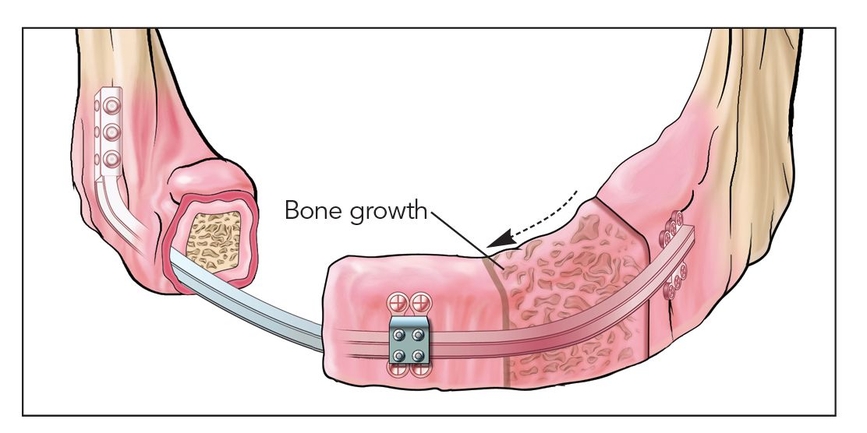
Fig 4-2c The transport segment moves (arrow) within the limits of periosteal tension.
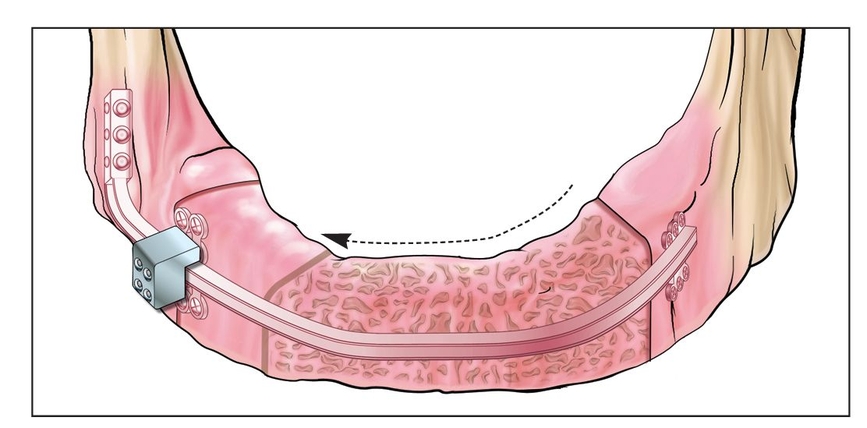
Fig 4-2d Following “docking” of the transport, the site is left to heal until there is osseous consolidation.
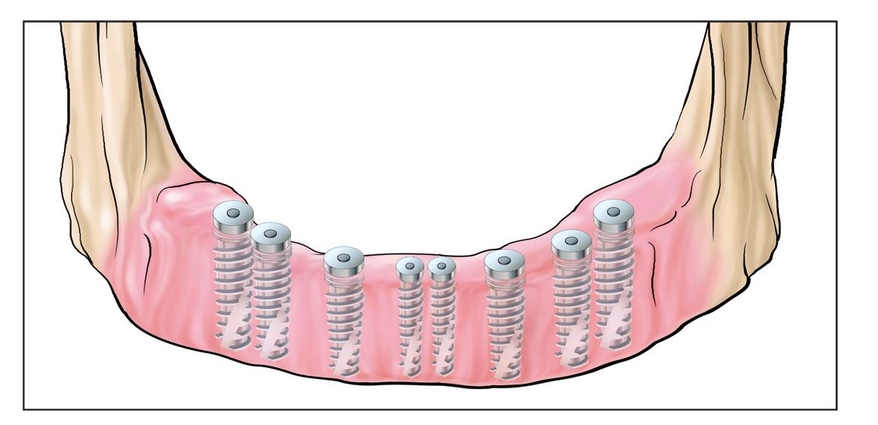
Fig 4-2e Plates and screws are removed following complete consolidation.
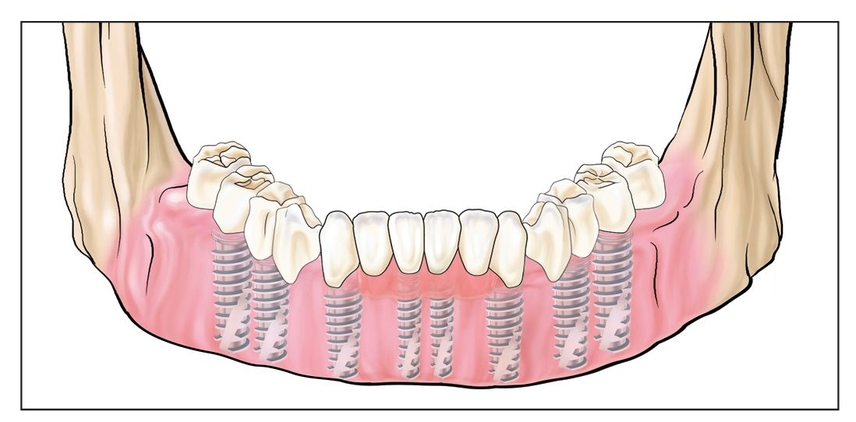
Fig 4-2f Finalization proceeds with implant placement and restorative dentistry.
 Case Reports
Case Reports
Case 1: Edentulous mandibular ridge inadequate in width to support a fixed denture
A 54-year-old woman with an edentulous mandible required a fixed denture (Fig 4-3a). A panoramic radiograph and computed tomograms (CTs) confirmed that the maximum height in the anterior region was 8.0 mm (Fig 4-3b). A vertical DO was planned in the area between the mental foramina to allow the placement of standard dental implants.
The previously described methods were used to perform an interforaminal periosteal incision and an osteotomy labially at 3 and 4 mm from the inferior border of the mandible, respectively. The transport segment was 6.0 cm wide and 4.0 mm high, with a 1.0-mm-long labial periosteal flap. The flap was repositioned and sutured, and a distraction device was adjusted and supraperiosteally fixed with positioning screws (Figs 4-3c and 4-3d). Special care was taken not to compress the underlying periosteum with plates. The transport segment was conformed to move within the limits of periosteal tension by 1.0-mm activation of the distraction device, and the open periosteum and the rest of the wound were closed in layers.
After a 7-day latency p/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


