Chapter 4
Primary Dentition Injuries
Aim
To provide a framework for the treatment of traumatic injuries to the primary dentition.
Outcome
After reading this chapter the reader should be aware of the appropriate treatment for the different types of injuries to primary teeth.
Aetiology
Injuries to the primary dentition are common. During its early development the permanent incisors are located palatally to and in close proximity with the apices of the roots of the primary incisors. When an injury occurs to a primary tooth, the force of the blow can readily be transmitted to the underlying permanent successor with risk of permanent damage to the permanent tooth.
The most accident-prone time in the primary dentition is between two and four years of age when infants are relatively unsteady on their feet and exploring. Realistically, this means that few restorative procedures will be possible. In the majority of cases the decision is between extraction or maintenance without performing extensive treatment. A primary incisor should always be removed if its maintenance will jeopardise the developing permanent tooth.
Diagnosis
This may be difficult with lack of cooperation of the child. Classification of injuries after examination is based on the WHO system shown in Table 1-1. The easiest radiographic examination method is an anterior oblique view using either a periapical or occlusal film (Fig 4-1).
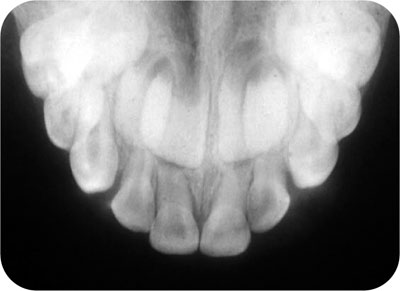
Fig 4-1 Anterior occlusal radiograph showing close relationship between primary teeth and permanent successors.
Treatment
This will be considered in terms of soft tissue injuries, tooth injuries and injuries to supporting alveolar bone.
Soft Tissue Injuries
These are covered in more detail in Chapter 3. They are common in primary dental trauma because the most common injury is displacement of the tooth. Treatment to the soft tissues is often very minimal and will most generally consist of:
-
debridement of the area with saline or 0.2% chlorhexidine
-
suturing (resorbable) if necessary under local analgesia
-
antibiotic cover for five days with amoxicillin (clindamycin if patient is allergic to amoxicillin), if the wound looks infected or was sustained outdoors
-
checking anti-tetanus status
-
having the parent clean the area with 0.2% chlorhexidine on cotton bud twice daily
-
recall every seven days until healed.
Tooth Injuries
Should the primary tooth be saved? Three factors need to be considered:
-
patient cooperation
-
parental attitude
-
possible damage to the underlying permanent teeth.
Treatment aims for primary teeth should be:
-
Prevent injury to the permanent successor
-
Save the primary tooth if this is compatible with the above aims
-
Restore the tooth to function with the least amount of treatment compatible with patient cooperation.
Crown and Root Fractures
Uncomplicated crown fracture
Either smooth sharp edges or restore with a resin-bonded restoration if patient cooperation is satisfactory.
Complicated crown fracture
Normally, extraction is the treatment of choice. Pulp extirpation and root canal filling with zinc oxide cement, followed by a resin-bonded composite is, however, possible with reasonable cooperation. Root canal treatment on primary incisors can be accomplished under a split rubber dam kept in place with rubber Wedjets (Hygenic). The pulp is extirpated and a working length radiograph taken. Gentle filing of the canal with 0.2% chlorhexidine irrigant should be completed to a working length 2 mm short of the radiographic apex. The canal can then be filled with a thin slurry of zinc oxide eugenol cement applied with a spiral filler. The access cavity should be sealed with a resin-bonded composite.
Crown-root fracture
The pulp is usually exposed and any restorative treatment is very difficult. The tooth is best extracted.
Root fracture
Without displacement and with only a small amount of mobility, the tooth should be kept under observation. If the coronal fragment becomes non-vital and symptomatic then it should be removed. The apical portion usually remains vital and undergoes physiological resorption with eruption of the permanent successor. Similarly, with marked displacement and mobility after a root fracture, only the coronal portion should be removed.
Concussion, Subluxation, and Luxation Injuries
Associated soft tissue damage should be cleaned by the parent twice daily with 0.2% chlorhexidine solution and cotton buds or gauze swabs until healing occurs.
Concussion
These injuries occur very commonly, but the infant is commonly not brought to a dentist until the tooth discolours, indicating loss of pulp vitality. Root canal treatment can be conducted as for a complicated coronal fracture.
Subluxation
If mobility is limited then the parents are advised to put the child on a soft diet for 1–2 weeks and to keep the traumatised area as clean as possible. Marked mobility requires/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


