Alignment and Occlusion of the Dentition
“OCCLUSION IS THE STATIC RELATIONSHIP OF THE TEETH AND IS BASIC TO ALL ASPECTS OF DENTISTRY.”
—JPO
THE ALIGNMENT AND OCCLUSION of the dentition are extremely important in masticatory function. The basic activities of chewing, swallowing, and speaking depend greatly not only on the position of teeth in the dental arches but also on the relationship of opposing teeth as they are brought into occlusion. Tooth positions are determined not by chance but by numerous controlling factors such as arch width and tooth size. They are also determined by various controlling forces such as those provided by the surrounding soft tissues. This chapter is divided into three sections. The first discusses the factors and forces that determine tooth position in the dental arches. The second describes the normal relationship of the teeth as they are aligned within the arches (intra-arch alignment). The third describes the normal relationship of the arches to each other as they are brought into occlusion (interarch alignment).
Factors and Forces Determining Tooth Position
The alignment of the dentition in the dental arches occurs as a result of complex multidirectional forces acting on the teeth during and after eruption. As the teeth erupt, they are directed into a position where opposing forces are in equilibrium. The major opposing forces that influence tooth position originate from the surrounding musculature. Labial to the teeth are the lips and cheeks, which provide relatively light but constant lingually directed forces. On the opposite side of the dental arches is the tongue, which provides labially and buccally directed forces to the lingual surface of the teeth. Both the forces applied labially by the lips and cheeks and lingually by the tongue are light but constant; these are the types of forces that, over time, can move teeth within the dental arches.
There is a tooth position in the oral cavity where the labiolingual and buccolingual forces are equal. This is the so-called neutral position or space, where tooth stability is achieved (Figure 3-1). If, during eruption, a tooth is positioned too far to the lingual or facial position, the prevailing force (the tongue if in linguoversion, the lips and cheeks if in facioversion) will force that tooth into the neutral position. This normally occurs when there is enough space for the tooth within the dental arch. If there is not enough space, the surrounding muscular forces are not usually sufficient to position the tooth in proper arch alignment. The tooth then remains outside the normal arch form and crowding is observed. This crowding remains until additional outside force is provided to correct the tooth size–arch length discrepancy (i.e., orthodontia).
Even after eruption any change or disruption in the magnitude, direction, or frequency of these muscular forces will tend to move the tooth into a position where the forces are again in equilibrium. This type of disruption may result if the tongue is either unusually active or large. This can result in greater forces applied lingually than labially to the teeth. The neutral space is not lost but merely displaced to the labial. This commonly leads to a labial flaring of the anterior teeth until they reach a position at which the labial and lingual forces are again in equilibrium. Clinically this presents as an anterior open bite (Figure 3-2, A). If an individual with this condition is asked to swallow, the tongue fills the anterior space, as shown in Figure 3-2, B. Originally it was assumed that the forces applied by the tongue during this type of swallow was responsible for the labial displacement or flaring of the anterior teeth. Recent evidence does not substantiate this concept. In fact, the greater likelihood is that the anterior teeth are being displaced labially by the constant resting or posturing position of the tongue and not the actual activity of swallowing.1 It is more likely that the tongue thrusting forward during a swallow is associated with the patient’s attempt to seal the mouth, as is necessary for efficient swallowing.

It is important to remember that these muscular forces are constantly acting on and regulating tooth function. Forces not directly derived from the oral musculature but associated with oral habits can also influence tooth position. Constantly biting on a pipe, for example, can alter tooth position. Musical instruments placed between the maxillary and mandibular teeth (e.g., a clarinet) may provide labial forces to the lingual surfaces of the maxillary anterior teeth, resulting in a labial flaring. When abnormal tooth position is identified, it is important to question the patient for these types of habits. Correction of the tooth position will surely fail if the etiology of the position is not eliminated.
The proximal surfaces of the teeth are also subjected to a variety of forces. Proximal contact between adjacent teeth helps maintain the teeth in normal alignment. A functional response of the alveolar bone and the gingival fibers surrounding the teeth appears to result in a mesial drifting of the teeth toward the midline. During mastication a slight buccolingual as well as vertical movement of the teeth over time also results in wear of the proximal contact areas. As these areas are worn, the mesial drifting helps maintain contact between adjacent teeth and thus stabilizes the arch. Mesial drift becomes most apparent when the surface of a posterior tooth is destroyed by caries or an entire tooth is extracted. With the loss of proximal contact, the tooth distal to the extraction site will drift mesially into the space, which (especially in the molar area) usually causes this tooth to tip into the space.
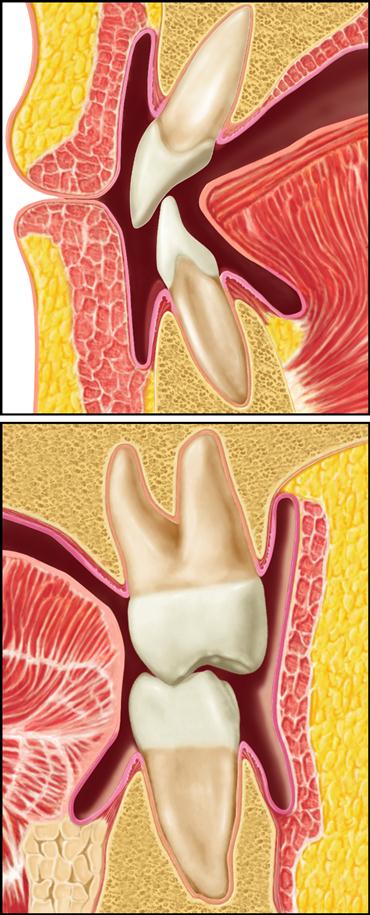
Another important factor that helps to stabilize tooth alignment is occlusal contact, which prevents the extrusion or supereruption of teeth, thus maintaining arch stability. Every time the mandible is closed, the unique occlusal contact pattern reemphasizes and maintains tooth position. If a portion of the occlusal surface of a tooth is lost or altered, the dynamics of the periodontal supportive structures will allow shifting of the tooth. Unopposed teeth are likely to supererupt until occlusal contact is established. Therefore when a tooth is lost, not only is the distal tooth likely to move mesially but the unopposed tooth is also likely to erupt, seeking an occlusal contact (Figure 3-3). It becomes apparent, therefore, that the proximal and occlusal contacts are important in maintaining tooth alignment and arch integrity. The effect of one missing tooth can be dramatic in terms of the loss of stability in the dental arches.
Intra-Arch Tooth Alignment
Intra-arch tooth alignment refers to the relationship of the teeth to each other within the dental arch. This section describes the normal intra-arch characteristics of the maxillary and mandibular teeth.
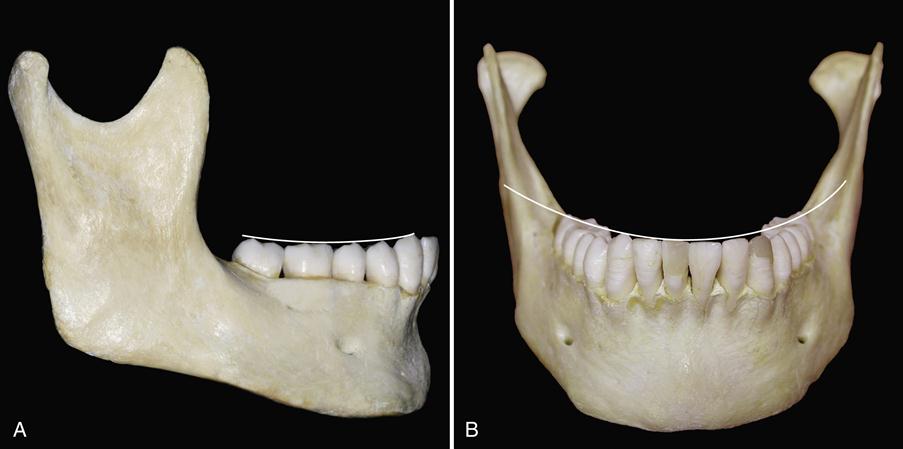
The plane of occlusion is the plane that would be established if a line were drawn through all the buccal cusp tips and incisal edges of the mandibular teeth (Figure 3-4) and then broadened into a plane to include the lingual cusp tips and continuing across the arch to include the buccal and lingual cups tips of the opposite side. The two temporomandibular joints (TMJs), which rarely function with identical simultaneous movements, determine much of the movement that is detectable. Because most jaw movements are complex, with the centers of rotation constantly shifting, a flat occlusal plane will not permit simultaneous functional contact in more than one area of the dental arch. Therefore the occlusal planes of the dental arches are curved in a manner that permits maximal utilization of tooth contacts during function. The curvature of the occlusal plane is primarily a result of the fact that the teeth are positioned in the arches at varying degrees of inclination.
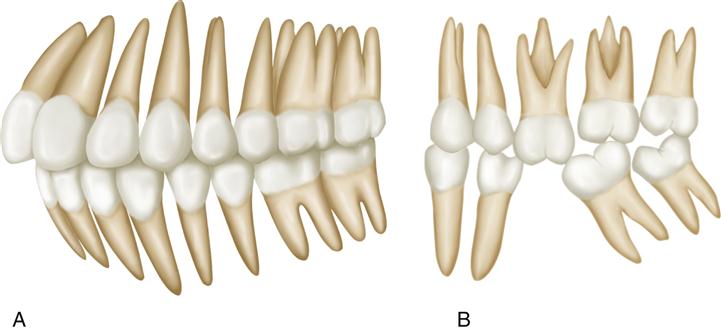
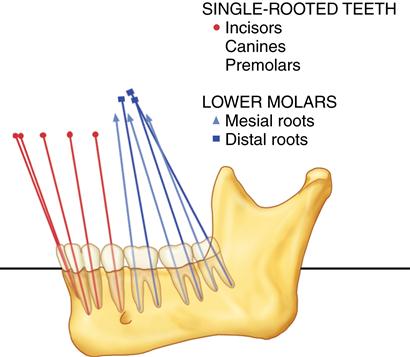
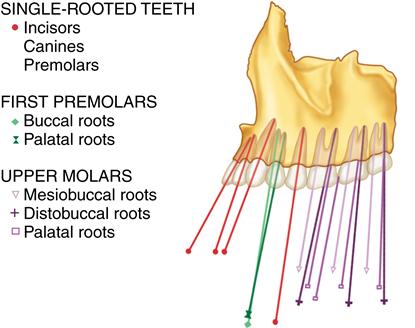
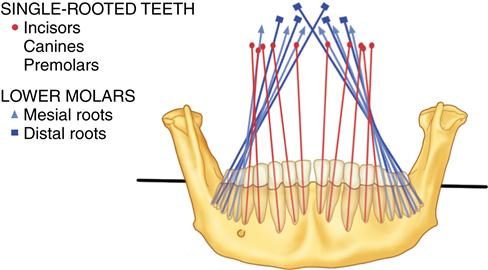
When the arches are examined from the lateral view, the mesiodistal axial relationship can be seen. If lines are extended through the long axes of the roots occlusally through the crowns (Figure 3-5), the angulation of the teeth with respect to the alveolar bone can be observed. In the mandibular arch, both the anterior and the posterior teeth are mesially inclined. The second and third molars are more inclined than the premolars. In the maxillary arch, a different pattern of inclination exists (Figure 3-6). The anterior teeth are generally mesially inclined, with the most posterior molars being distally inclined. If, from the lateral view, an imaginary line is drawn through the buccal cusp tips of the posterior teeth (molars and premolars), a curved line following the plane of occlusion will be established (see Figure 3-4, A) that is convex for the maxillary arch and concave for the mandibular arch. These convex and concave lines match perfectly when the dental arches are placed into occlusion. This curvature of the dental arches was first described by Von Spee2 and is therefore referred to as the curve of Spee.
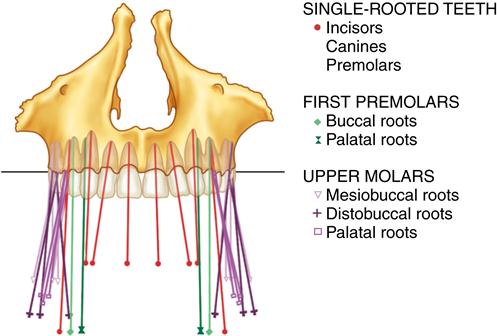
When the dental arches are observed from the frontal view, the buccolingual axial relationship can be seen. Generally the posterior teeth in the maxillary arch have a slightly buccal inclination (Figure 3-7). In the mandibular arch, the posterior teeth have a slightly lingual inclination (Figure 3-8). If a line is drawn through the buccal and lingual cusp tips of both the right and the left posterior teeth, a curved plane of occlusion will be observed (see Figure 3-4, B). The curvature is convex in the maxillary arch and concave in the mandibular arch. Again, if the arches are brought into occlusion, the tooth curvatures will match perfectly. This curvature in the occlusal plane observed from the frontal view is called the curve of Wilson.
Early in dentistry, observers sought to develop some standardized formulas that would describe intra-arch relationships. Bonwill,3 one of the first to describe the dental arches, noted that an equilateral triangle existed between the centers of the condyles and the mesial contact areas of the mandibular central incisors. He depicted this as having 4-in. sides. In other words, the distance from the mesial contact area of the mandibular central incisor to the center of either condyle was 4 in. and the distance between the centers of the condyles was 4 in. In 1932 Monson4 utilized Bonwill’s triangle and proposed a theory that a sphere existed with a radius of 4 in. whose center was an equal distance from the occlusal surfaces of the posterior teeth and the centers of the condyles. Although these concepts were roughly correct, they were oversimplifications and would not hold true in all instances. Reaction to such simplistic theories stimulated investigators to both oppose and defend them. From such controversies developed the theories of occlusion that are used in dentistry today.
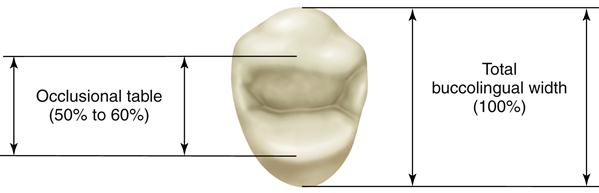
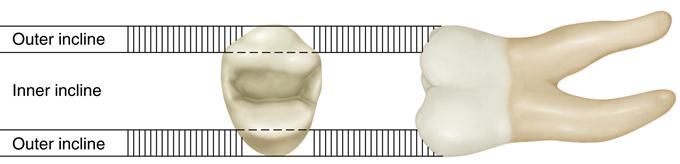
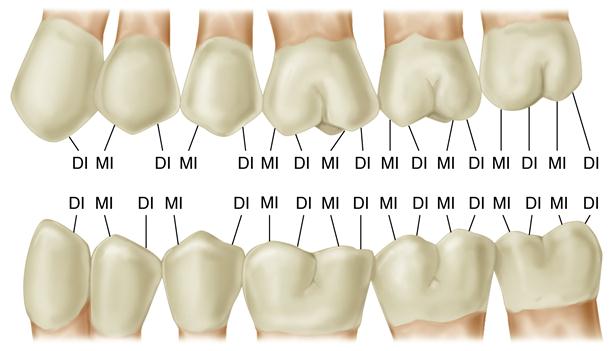
The occlusal surfaces of the teeth are made up of numerous cusps, grooves, and sulci. During function these occlusal elements permit effective breaking up of the food and mixing with saliva to form a bolus that is easily swallowed. The occlusal surfaces of the posterior teeth can be divided for discussion purposes into several areas. The area of the tooth between the buccal and lingual cusp tips of the posterior teeth is called the occlusal table (Figure 3-9). The major forces of mastication are applied on this area. The occlusal table represents approximately 50% to 60% of the total buccolingual dimension of the posterior tooth and is positioned over the long axis of the root structure. It is considered the inner aspect of the tooth, since it falls between the cusp tips. Likewise the occlusal area outside the cusp tips is called the outer aspect. The inner and outer aspects of the tooth are made up of inclines that extend from the cusp tips to either the central fossa areas or the height of the contour on the lingual or labial surfaces of the teeth. Thus these inclines are called inner and outer inclines (Figure 3-10). The inner and outer inclines are further identified by describing the cusp of which they are a part. For example, the inner incline of the buccal cusp of the maxillary right first premolar identifies a very specific area in the dental arch. Tooth inclines are also identified with respect to the surface toward which they are directed (i.e., mesial or distal). Mesially inclined surfaces are those that face the mesial portion of the tooth, and distally inclined surfaces face the distal portion (Figure 3-11).
Interarch Tooth Alignment
Interarch tooth alignment refers to the relationship of the teeth in one arch to those in the other. When the two arches come into contact, as in mandibular closure, the occlusal relationship of the teeth is established. This section describes the normal interarch characteristics of the maxillary and mandibular teeth in occlusion.
The maxillary and mandibular teeth occlude in a precise and exact manner. A line that begins at the distal surface of the third molar, extends mesially through all of the proximal contact areas around the entire arch, and ends at the distal surface of the opposite third molar represents the arch length. Both arches have approximately the same length, with the mandibular arch being only slightly smaller (maxillary arch, 128 mm; mandibular arch, 126 mm).5 This slight difference is a result of the narrower mesiodistal distance of the mandibular incisors compared to the maxillary incisors. The arch width is the distance across the arch. The width of the mandibular arch is slightly less than that of the maxillary arch; thus when the arches occlude, each maxillary tooth is more facially positioned than the occluding mandibular tooth.
Since the maxillary teeth are more facially positioned (or at least have more facial inclination), the normal occlusal relationship of the posterior teeth enables the mandibular buccal cusps to occlude along the central fossa areas of the maxillary teeth. Likewise the maxillary lingual cusps occlude along the central fossa areas of the mandibular teeth (Figure 3-12). This occlusal relationship protects the surrounding soft tissue. The buccal cusps of the maxillary teeth prevent the buccal mucosa of the cheek and lips from falling between/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


