Complications of Local Flaps
Introduction
Complications associated with surgery are perhaps nowhere more apparent and devastating than when they occur on the face. Conley spoke of surgical complications by saying, “These untoward events, unpredictable and unwanted, lurk in all surgical arenas, in the biological process and in the patient. They give credence to our frailty, from which there is no escape.”1 It is essential that all facial surgeons become familiar with the potential complications associated with facial reconstructive surgery. Furthermore, it is of utmost importance that surgeons anticipate these undesirable events and take proper measures to help prevent their occurrence.
Establishing a consistent perioperative routine is the first step in preventing complications. Appropriate preoperative counseling of the patient will reduce the likelihood of complications. Informed consent should include an open discussion of potential problems that may occur. Hand scrubbing, sterile surgical attire, and surgical site preparation are important in reducing the likelihood of infection.2–6 Immediate and regular postoperative evaluations of the patient will facilitate early recognition and treatment of complications. Some complications are reversible, and expeditious treatment may prevent a reversible complication from becoming an irreversible one. This chapter discusses complications inherent to surgery, those related to the medical conditions of patients, and complications associated with surgical technique and local flap design.
Complications Inherent to Surgery
Adherence to well-established surgical principles is essential for minimizing the incidence of complications in performing facial reconstructive surgery. Conley writes that “hemostasis should be absolute … all flaps should be viable and tissue should not be closed with undue wound closure tension. The type and size of the suture material should be appropriate for the job it has to do. Compliance with these fundamental principles establishes the groundwork for healing … the incidence of complications will develop in direct proportion to the violation of these principles.”1
Bleeding
The most common causes of bleeding from facial reconstruction with local flaps are drug-associated coagulopathy and inadequate hemostasis.7 Patients are questioned preoperatively concerning use of all prescription and over-the-counter medications that may contribute to perioperative bleeding. All aspirin-containing products, nonsteroidal anti-inflammatory medicines, vitamin E, and most herbal remedies are discontinued 1 week or more before surgery. The exception to this policy is patients with cardiac stents. These patients continue to take aspirin if it is prescribed by their cardiologist. Cold and sinus medications are avoided because many contain substances that may affect clotting or cause adverse elevation in blood pressure. Discontinuation of any medications prescribed by a physician to reduce blood clotting is coordinated with the patient’s primary physician or cardiovascular specialist. Bleeding may also be associated with hypertensive events, hepatic or renal failure, vomiting, straining, or alterations in the hematopoietic system.
Hematomas may cause compromise of local flap vascularity by inducing vasospasm, stretching the subdermal plexus, or separating the flap from the surface of the recipient site.8–10 Furthermore, iron compounds in a hematoma may promote free radical production, leading to flap necrosis.11,12 Hematoma formation also predisposes to infection, which may compromise flap vascularity secondary to inflammatory edema.13,14
If a hematoma occurs, patients usually complain of significant pain. The wound may appear mottled, pale, or bluish, and palpation of the skin in the area of the hematoma usually reveals a tight, tense flap with oozing of blood from the suture lines. Small (5-10 mL) hematomas may sometimes be aspirated through the suture line by use of a 25-mL syringe attached to an 18-gauge needle. A compression dressing is then applied and the patient is re-examined in 24 to 48 hours. If the hematoma recurs, it may be necessary to return the patient to the operating room to properly drain it. There, the wound is opened at a dependent portion, the hematoma is evacuated, and bleeding vessels are controlled. A compression dressing is reapplied. The patient is examined within 24 hours. Expediency in treatment of large hematomas is essential to avoid compromise of flap vascularity and skin slough. Typically, within the first 48 hours after surgery, hematomas consist of a fresh clot of gel or liquid consistency. As the clot matures during the next several days, it becomes firmer and adherent to the underlying wound bed and cannot be easily aspirated. After approximately 2 weeks, fibrinolysis begins, and the hematoma liquefies (Fig. 26-1). At this point, repeated aspiration or drainage may be necessary to facilitate adherence of the flap to the wound bed (Fig. 26-2).

FIGURE 26-1 A, Rotation flap designed to repair 5 × 4-cm cutaneous defect of the temple. Partial primary wound closure was also planned at superior aspect of defect. Repair of smaller skin defect occurring in area of anticipated standing cutaneous deformity of rotation flap is noted. B, Wound repaired. C, Postoperative result at 2 weeks. Flap necrosis at peripheral border may have been related to development of hematoma at the base of flap. (Courtesy of Shan R. Baker, MD.)

FIGURE 26-2 A, Midface soft tissue and bone defect after resection of skin malignant neoplasm. B, Hematoma developed 1 week postoperatively, after restarting of anticoagulant medication (warfarin). C, One month after evacuation of hematoma. Lower eyelid retraction noted. Massage of lower eyelid initiated. D, Postoperative result at 6 months.
Injury of Adjacent Anatomic Structures
Sensory nerves are also susceptible to injury during facial reconstructive procedures. Extensive undermining along the superior bony orbital rim may injure the supraorbital and supratrochlear nerves, leading to dysesthesias in their sensory distributions.15 Similarly, the deep branch of the supraorbital nerve runs within the galea aponeurotica and may be injured when the frontalis muscle is undermined in the subgaleal plane while defects of the lateral forehead skin are being closed. The infraorbital and mental nerves are less susceptible to injury but may be compromised during dissection in their respective areas. The great auricular nerve may be injured during subcutaneous dissection in the periauricular area. This nerve is identified and preserved when skin is dissected away from its attachment to the superior aspect of the sternocleidomastoid muscle.
Injury to eyelid structures may lead to devastating consequences, including lagophthalmos, lacrimal duct obstruction, visual field obstruction, and vision loss. Facial surgeons should be familiar with the cross-sectional anatomy of the upper and lower eyelids, especially the connective tissue support apparatus and the position and location of the levator muscle. Injury to these structures is best avoided because treatment is extremely difficult if scarring has occurred.
Infection
Fortunately, infection during facial surgery is reported to be as low at 2.8%, perhaps secondary to the rich vascularity of facial tissues.16–20 However, the infection rate associated with facial flaps is increased in certain circumstances. Higher infection rates are associated with wounds that are repaired in a delayed fashion, as is often the case with facial flaps used to repair wounds created by micrographic surgery.21 Ischemia of flaps is likely to increase the risk for infection because tissue oxygenation is extremely important in prevention of wound bacterial colonization.16,22,23
Wound infection is associated with poor outcomes. Infection of a cutaneous flap is usually associated with distortion from inflammatory edema. Release of toxic substances and free radicals from inflammatory mediators leads to decreased collagen production and early degradation of suture materials with potential wound dehiscence. Necrosis of all or part of the flap may develop, with the final scar being widened or thickened. Systemic dissemination of bacteria may occur if wound infections are not treated promptly.24
Although perioperative antibiotic prophylaxis is controversial in clean wounds, it has been shown to be effective in decreasing wound infection rates when it is used for clean-contaminated wounds.16,21,22 Antiseptic solutions for skin preparation, sterile technique, proper scrubbing, and surgical attire are key elements in helping prevent infection. It is also important to avoid crushed, charred, or excessively thinned tissue. Staphylococcus aureus is the most common single pathogen causing wound infections, but streptococci, gram-negative bacteria, and oral anaerobes may also be isolated from infected wounds.21 The author uses parenteral antibiotics when mucosal surfaces are incised, when cartilage grafting is performed, and during ear reconstruction to help prevent perichondritis. They are also employed in patients with underlying medical conditions that may predispose to infection, such as diabetes and immunosuppression. In these cases, a preoperative dose of intravenous cephalosporin is administered, followed by 5 days of an oral cephalosporin. In penicillin-allergic patients, clindamycin is used. In patients with open wounds older than 3 days, a 5-day course of oral cephalosporin is recommended before the surgical repair. This will decrease the bacterial colonization of the granulation tissue that has developed in the depths of the wound.
Excessive pain or erythema at the wound site may herald an infection (Fig. 26-3). These clinical signs usually appear between the fourth and eighth days after wound closure. Topical allergies to antibiotic ointments and creams applied to the wound may be confused with wound infection. Topical allergic reactions are manifested as erythema, often with vesicle formation and exudates forming on all areas treated with the topical medication (Fig. 26-4). Treatment consists of discontinuation of the offending agent and cleaning of the wound with soap and water to remove all residual topical medication.

FIGURE 26-3 A, B, Infected nasal wound after contouring procedure to correct trap-door deformity of bilobe nasal flap. (Courtesy of Shan R. Baker, MD.)

FIGURE 26-4 Topical allergic reaction to antibiotic ointment causing erythema and vesicles of skin. (Courtesy of Shan R. Baker, MD.)
If a wound infection does develop, Gram stain and culture of any drainage from the wound are performed. The patient is treated with an appropriate broad-spectrum antibiotic until culture results and sensitivities are available. Any wound fluctuance is drained and the wound irrigated. Significant fluid collections beneath a cutaneous flap usually require the placement of a drain or wick to facilitate further drainage and adherence of the flap to the underlying wound bed. The presence of excessive granulation tissue may require débridement to reduce the bacterial load. Topical antibiotic preparations may also be employed, and superficial sutures are removed to eliminate foreign bodies in the wound.25 Open wounds are allowed to heal by secondary intention. The resulting scar is addressed at a later time once the infection has been adequately treated and scarring has matured.
Viral and fungal infections of facial wounds are rare and almost always are associated with skin resurfacing procedures, such as dermabrasion and laser peels. Although these infections may occur anywhere on the face where resurfacing has been performed, they occur predominantly in the area of the lips when this facial region is treated (Fig. 26-5). Patients undergoing dermabrasion or laser treatment to scars of the lip should receive antiviral therapy before treatment and postoperatively until the treated area has completely re-epithelialized.

Abnormal Scarring
Patients with darker skin and those with a family history of excessive scarring are prone to the development of hypertrophic scars and keloids after surgery. Although numerous treatment modalities have been proposed, there is no definitive method of managing or preventing these problems.26 Intralesional triamcinolone acetonide (10 mg/mL) is often helpful in reducing the volume of scar tissue within a hypertrophic or keloid scar. If the scar is responsive to the injections, surgical excision may be performed after a preoperative injection 1 week before surgery. Several injections are usually required postoperatively every 2 months after excision of the scar for an indeterminate time interval (Fig. 26-6). Rarely, irradiation is considered for extremely problematic keloids.

FIGURE 26-6 A-D, Preoperative views and postoperative result 1 year after keloid excisions. Postoperative injection of triamcinolone acetonide (10 mg/mL) into the surgical site was performed every 2 months. (Courtesy of Shan R. Baker, MD.)
Glucocorticoids have a profound anti-inflammatory effect. The most common form used is triamcinolone acetonide suspension, which is injected into the depths of the scar. Injections are used to soften firm scars, to lower raised keloids, and to prevent their recurrence. Steroids decrease fibroblast proliferation, reduce blood vessel formation, and interfere with fibrosis by inhibiting extracellular matrix protein gene expression. When steroid injection is used at the time of keloid excision, it is injected at the wound margins immediately after excision. Repeated injection is performed at 3- to 6-week intervals. Multiple injections are usually necessary. Excessive steroid injection of scars may lead to skin atrophy, hypopigmentation, and telangiectasia (Fig. 26-7).

FIGURE 26-7 Skin atrophy with telangiectasia after steroid injection of scar. (Courtesy of Shan R. Baker, MD.)
Scar hyperpigmentation may be seen in patients who tan easily, particularly if the patient has excessive sun exposure during the immediate postoperative period. Hyperpigmentation improves over time and with sun avoidance. Use of topical hydroquinone gel with or without the administration of an anti-inflammatory drug may be helpful in preventing permanent discoloration of the scar (Fig. 26-8).


Wound Dehiscence
Wound dehiscence may develop secondary to infection, hematoma, or skin necrosis (Fig. 26-9). In addition, dynamic motion or trauma to wounds may also lead to wound separation. Typically, wounds have 3% to 5% of normal skin tensile strength at 2 weeks after surgery, emphasizing the need for subcutaneous sutures. At 1 month, only 35% of the maximum wound tensile strength has been gained. However, at this point, the wound is usually able to withstand the forces of normal physical activity. During the succeeding months, wound tensile strength increases to 80% of the strength of normal tissue. Wound separations in uncomplicated, clean wounds may be repaired with sutures if this is performed within 24 hours of wound dehiscence. Wound separations that have been present for more than 24 hours are best left to heal by secondary intention, with scar revision reserved for the future if necessary.24,27

Medical Conditions
Patients are questioned preoperatively concerning their use of tobacco and alcohol. Heavy alcohol consumption will dilate blood vessels, predisposing to hematoma formation. Avoidance of alcohol during the perioperative period is recommended. Ideally, tobacco and nicotine products should be avoided, at least 4 to 8 weeks before and after surgery. Even smoking cessation for 2 days before surgery and 7 days after surgery has been shown to have beneficial effects on flap survival.28 Smokers develop skin necrosis three times more frequently than nonsmokers do, and the extent and depth of skin slough are more severe.28 Nicotine causes systemic vasoconstriction through activation of the adrenergic nervous system, which may lower tissue oxygenation pressure by more than 50%. This occurs within 10 minutes of smoking a cigarette and lasts approximately 50 minutes. Smoking also produces carbon monoxide, which has a higher affinity for hemoglobin than oxygen, thereby producing high levels of carboxyhemoglobin.29–33 This means that less oxygen can be delivered to the tissues by the vascular system. When possible, consideration is given to delaying surgical procedures until smoking cessation can be ensured.
Surgical Technique and Flap Design
Ischemia
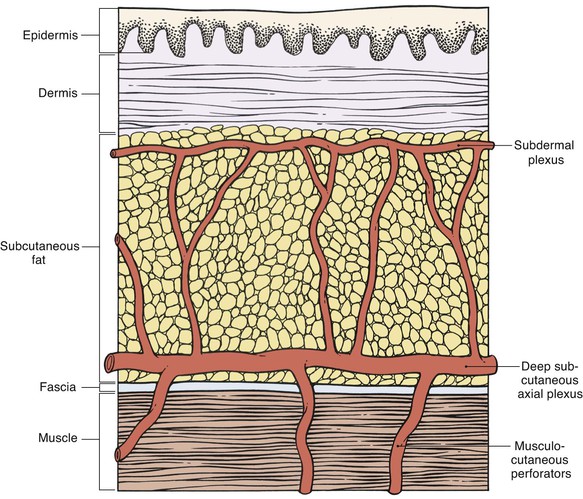
Appropriate flap design is essential to ensure sufficient perfusion pressure of the entire flap.34 According to their vascularity, local and regional flaps may be classified as random pattern or axial pattern flaps. Flap dissection should proceed at the appropriate tissue depth to preserve the blood supply to the skin (Fig. 26-10). Random pattern flaps require an intact subdermal plexus, and dissection is performed in the subcutaneous tissue plane. Too superficial dissection or improper flap design may lead to compromise of the flap’s vascularity. Random patterned flaps have a critical length beyond which the perfusion of the distal flap does not occur. Although increasing the width of a flap’s pedicle potentially increases the number of vessels contained in the subdermal plexus of the flap, it does not increase the perfusion pressure to the distal portion of the flap. Therefore, within certain limits, widening the pedicle does not increase the survival of the distal flap. Axial pattern flaps are nourished by a named artery that is located within the tissues of the flap and is parallel to the linear axis of the flap.
Design of axial pattern flaps requires a thorough knowledge of the location and orientation of the arterial vessels supplying the skin of the donor area to properly align the flap with the axis of the artery and to avoid inadvertent injury to the flap’s blood supply. Careful dissection is performed around the flap’s pedicle. Increasing the width of the pedicle of axial flaps does not necessarily improve perfusion.35,36 In fact, it is more prudent to raise a thicker flap that contains deeper subcutaneous vessels than to design the flap with a wider base (Fig. 26-11). An excessively wide pedicle may also complicate the use of the donor site for repair of future defects (Fig. 26-12).
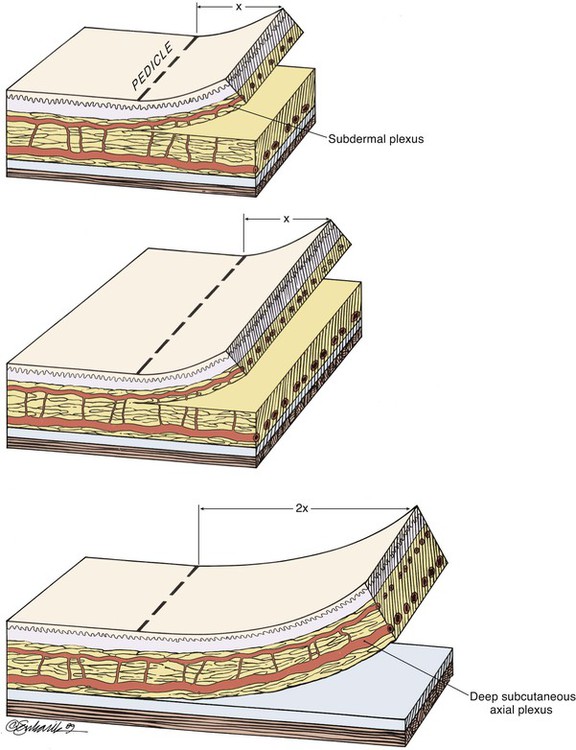
FIGURE 26-11 Widening pedicle of flap does not increase distal flap perfusion, but increasing thickness of flap to include deeper, larger vessels does.

Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


