2
Soft Tissue Head and Neck Pathology Description and Documentation
There are five main descriptive features of head and neck soft tissue pathology1:
- Site
- Morphology
- Color
- Size
- Consistency
A complete and accurate description of these features is required for concise and specific documentation of the observed soft tissue pathology. Failure to do so is tantamount to a potential failure of risk management for the dental practitioner.
It is critical to determine and document as precisely as possible the specific anatomical location from which the pathology arises (i.e., epicenter) as well as the other single, or multiple, additional component(s) of the disease process. The overall shape(s) and morphology(ies) of the lesion must be determined by a combination of visual examination and digital palpation. There are three basic morphological types:
- Elevated—surface is above the normal plane of the mucosa.
- Depressed—surface is below the normal plane of the mucosa.
- Flat—surface is level with the normal plane of the mucosa.
The sole hue, or the predominant hue and additional hues, of the lesion must be assessed and recorded in the dental record. The lesion’s size, expressed in metric system units (length and width at their greatest dimension and, in some cases, height), must be documented. As noted in the section “Morphology of Lesions,” some morphological terms’ definitions include a measurement, which is an additional reason to determine the pathology’s size. Lastly, by digital palpation of the lesion, the consistency and surface topography are evaluated and recorded. The clinician should record all of these descriptors of the soft pathology lesion with the mindset that this information will be conveyed to another person without that person having the benefit of ever seeing the lesion. Thus, precise and extremely accurate clinical descriptions must be recorded for the benefit of the patient’s clinical differential diagnosis and resultant planned treatment and/or management of the soft tissue lesion. There is no excuse for a dental practitioner who fails to do this important and fundamental initial prediagnostic step.
Anatomical Site of Lesions
The exact anatomical site or sites that a soft tissue lesion(s) occupies is critical for the medicolegal record and diagnostic process. The following is a partial list of potential sites of the oral cavity proper, oropharynx, and immediate adjacent cutaneous structures. For additional anatomic sites the clinician is referred to numerous excellent head and neck anatomy texts. The clinician should always refrain from using colloquial or layman’s terms for these sites when entering them in a medicolegal document. Accurate and effective patient communication is important; however, terms such as buccal gutter, gums, cheeks, and roof of mouth are inappropriate entries in a dental chart.
- Perioral skin—left; right; bilateral; upper; lower
- Lip—left; right; bilateral; upper; lower
- Vermilion border
- Wet–dry line, not including the wet (i.e., labial mucosa)
- Commissure (angle)
- Skin of lip
- Oral cavity proper—left; right; bilateral
- Tongue
- Dorsum, anterior/posterior
- Lateral, anterior/posterior
- Ventral, anterior/posterior
- Floor of mouth
- Sublingual plica and caruncle
- Lingual frenum
- Wharton’s ducts
- Gingiva, anterior/posterior
- Attached
- Marginal (free)
- Interdental papillae (between teeth #’s _ and _)
- Location
- Labial
- Facial
- Buccal
- Palatal
- Edentulous alveolar ridge (see number 6)
- Vestibule/mucobuccal fold
- Maxillary—anterior/posterior
- Mandibular—anterior/posterior
- Buccal mucosa (mucous membrane cheek)
- Occlusal plane
- Superior
- Inferior
- Anterior, middle, and posterior one-thirds
- Stensen’s duct
- Occlusal plane
- Edentulous alveolar ridge mucosa
- Maxillary, anterior/posterior
- Mandibular, anterior/posterior
- Retromolar pad
- Trigone area
- Hamular notch
- Maxillary tuberosity
- Hard palate
- Palatine papilla
- Midline
- Lateral
- Junction with soft palate
- Tongue
- Oropharynx—left; right; bilateral
- Soft palate
- Uvula
- Lateral
- Anterior tonsillar pillar
- Tonsil and fossa (pharyngeal tonsil)
- Posterior tonsillar pillar
- Posterior pharyngeal wall
- Base of tongue
- Posterior and lateral walls
- Soft palate
Morphology of Lesions
Elevated Lesions
Blisterform
Blisterform lesions contain a bodily fluid and are usually referred to by the layman as a “blister.” They are usually identified by a characteristic translucent appearance and upon palpation feel soft, with a variable amount of rebound and a fluctuant sensation. They are given specific descriptive names depending on their greatest diameter and the type of fluid material contained.
- Vesicle (Fig. 2.1a)—equal to or less than 0.5 cm (5 mm) in greatest diameter. A vesicle contains serum or mucin, and the color is usually clear or translucent; however, it is sometimes slightly whitish or bluish.
- Bulla (Fig. 2.1b)—greater than 0.5 cm in greatest diameter. A bulla usually contains serum or mucin but may occasionally contain extravasated blood; the color may be clear, reddish, or bluish depending on the fluid content.
- Pustule (Fig. 2.1c)—any size. A pustule exclusively contains a purulent exudate (“pus”) and the color is yellowish.
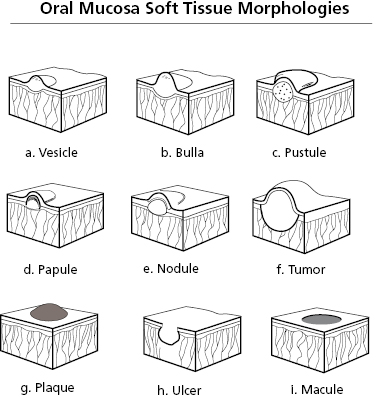
Nonblisterform
Nonblisterform lesions are solid and thus have no fluid component; they are opaque and feel firm upon palpation. They are given specific descriptive names depending on their diameter and pattern.
- Papule (Fig. 2.1d)—consists of tissue and is equal to or less than 0.5 cm in greatest diameter.
- Nodule (Fig. 2.1e)—consists of tissue and is greater than 0.5 cm but equal to or less than 2.0 cm in largest diameter.
- Sessile—broad-based. The greatest diameter is at the base.
- Pedunculated—connected to the surface by a stalk. The greatest diameter is above the base.
- Tumor (Fig. 2.1f)—consists of tissue and is greater than 2 cm in greatest diameter. A tumor is usually sessile but can be p/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


