CHAPTER 15
Sinus Floor Intrusion As a Vascularized Osteoperiosteal Flap
Growth is barely controlled damage.
—James Richardson
Patients who are edentulous in the posterior maxilla often display enlarged sinuses and reduced alveolar bone height. Treatment modalities for patients with inadequate bone depend on the volume of residual bone, the morphology of the alveolar crest, and the amount of space available for a prosthesis.1 The sinus lift procedure, first described by Boyne and James,2 has been used successfully to augment the sinus floor. The surgeon creates a lateral window, gently lifts the sinus membrane, and then grafts the sinus floor. Indirect techniques in which an osteotome is used from a crestal approach to intrude the maxillary sinus floor have been used in patients with inadequate height in the posterior maxilla. These indirect techniques were developed to provide an alternative to direct sinus elevation and thereby reduce surgical manipulation.
An aim of the osteotome technique is to increase the density and volume of bone at the apical portion of the osteotomy site through compression.3 The osteotome technique, originally reported by Summers,3 takes advantage of the fact that bone is viscoelastic and can be compressed and manipulated. Bone compaction, cortical sinus floor elevation, and ridge expansion can be performed with this technique. The minimum alveolar bone height recommended for the osteotome technique is 5 mm.4,5
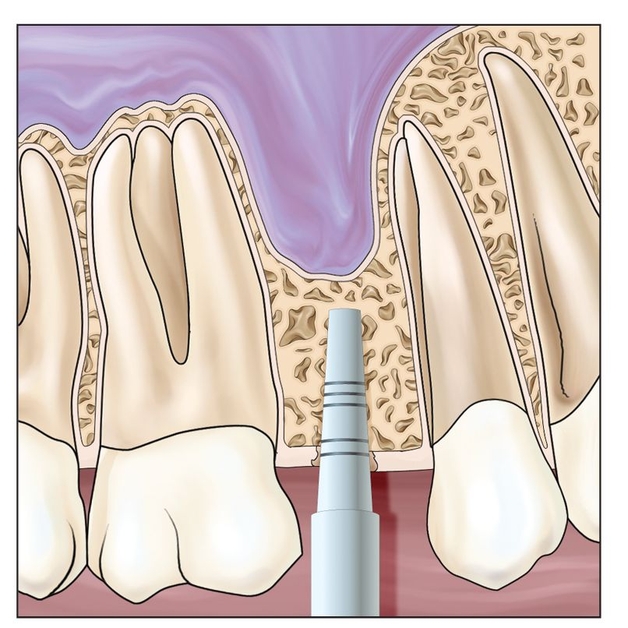
Fig 15-1a Osteotomes are used to gradually enlarge the osteotomy.
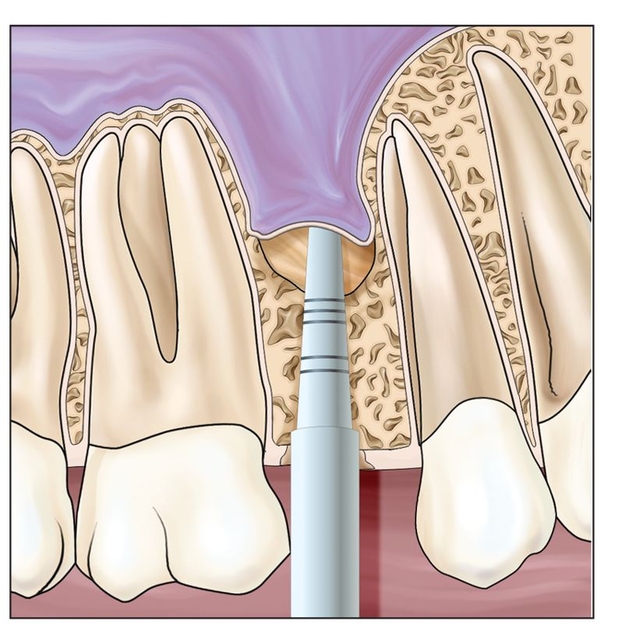
Fig 15-1b The sinus floor is gently intruded.
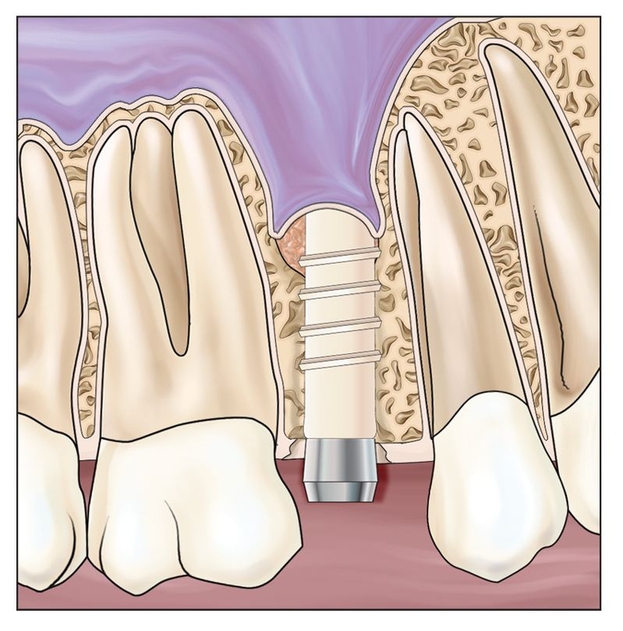
Fig 15-1c An implant is placed following sinus elevation and grafting.
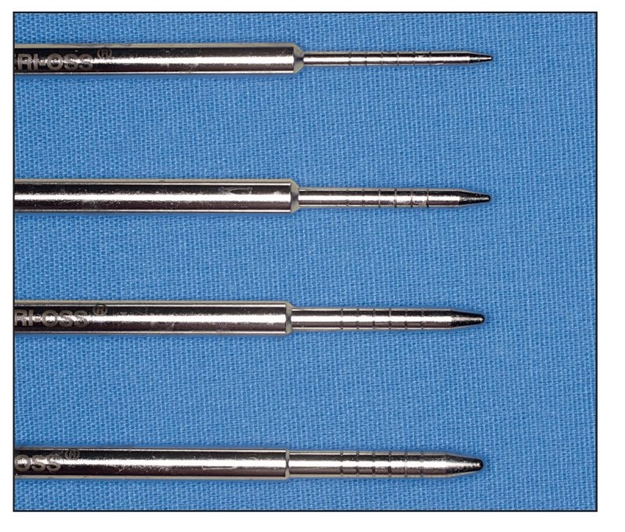
Fig 15-2 Osteotomes of increasing diameter are used to expand the alveolar bone.
 Surgical Technique
Surgical Technique
This surgical technique can be performed with or without elevation of a mucoperiosteal flap. An initial osteotomy is performed with either a drill or osteotome (Fig 15-1). A small-diameter osteotome is used to reach and infracture the sinus floor. The tips of the osteotomes have a concave nose and a sharpened edge, which can be used to scrape bone from the side wall of the osteotomy. Increasingly larger osteotomes are then used to expand the alveolar bone in the buccal-lingual and apical-coronal directions (Fig 15-2).
The harvested bone, graft material, and trapped fluids create pressure as the osteotomes are inserted, resulting in elevation of the sinus floor. Care is taken to avoid perforation of the sinus membrane. Prior to implant placement, the cavity is rinsed with saline, and any membrane perforations are noted. If graft material is to be used, it is placed before the dental implants (Figs 15-3 to 15-5).
A goal is to remain short of the sinus membrane during the initial implant site preparation (Fig 15-6). Precise treatment planning is important to allow the clinician to stop 1 to 2 mm inferior to the sinus floor. Tearing of the sinus floor is more likely to result from drilling the osteotomy to the floor than it is from elevating a segment of bone with the sinus membrane attached. Imaging is helpful to rule out the presence of sinus pathology, to locate septa, and to determine the height of the alveolar bone more accurately.
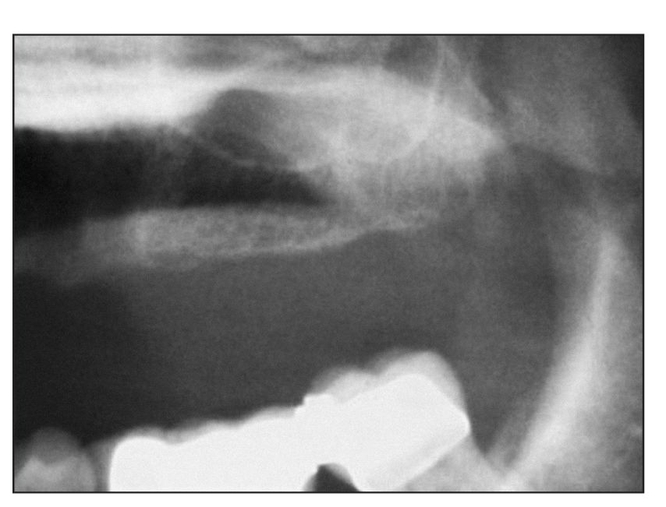
Fig 15-3 A patient may have inadequate bone for implant placement from premolar to molar sites.
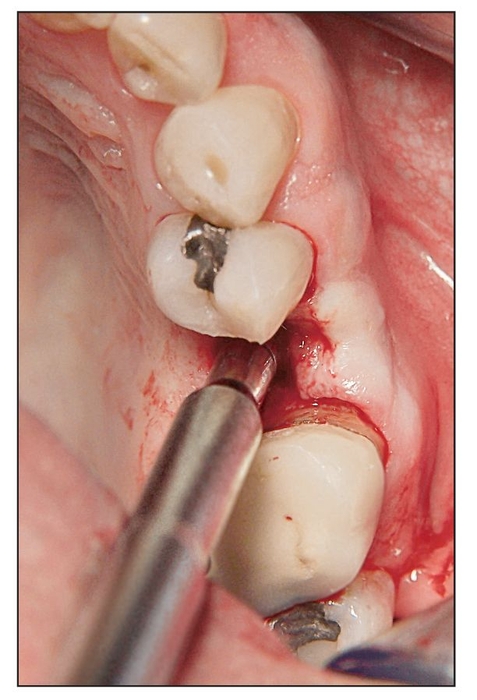
Fig 15-4 An osteotome is used to expand the osteotomy in a premolar site.
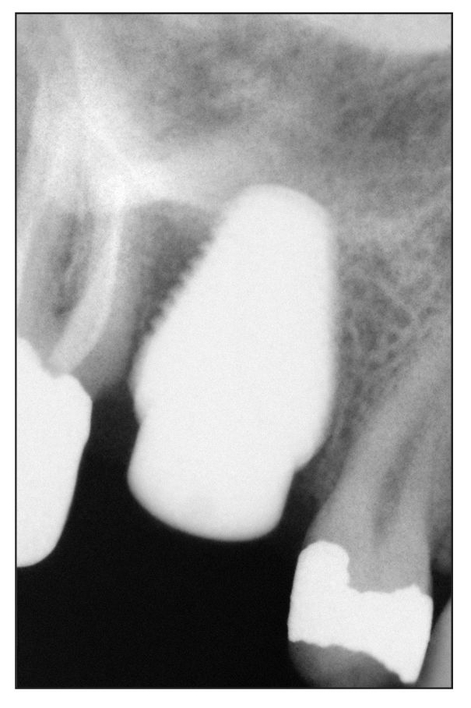
Fig 15-5 The postoperative radiograph shows the elevated sinus floor in a molar site.
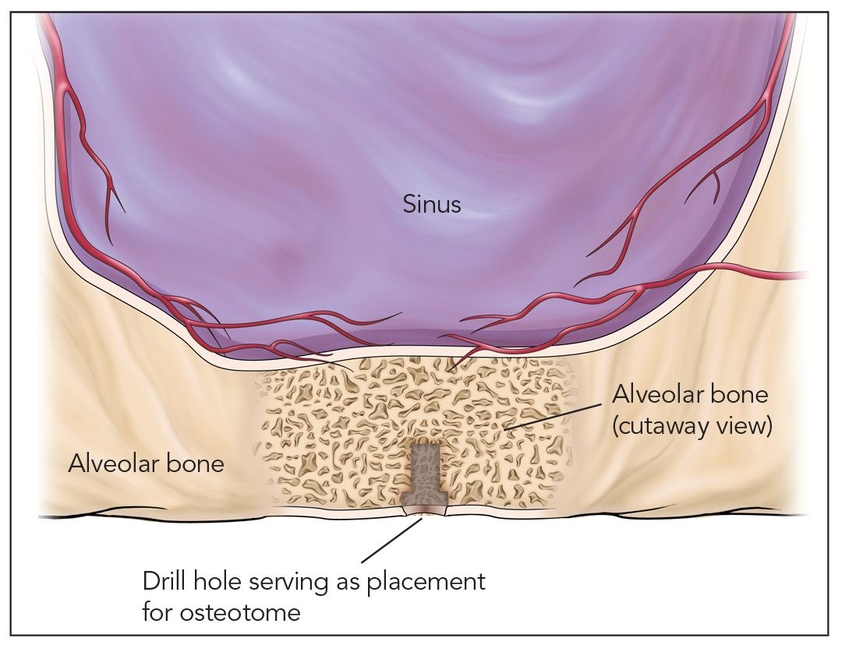
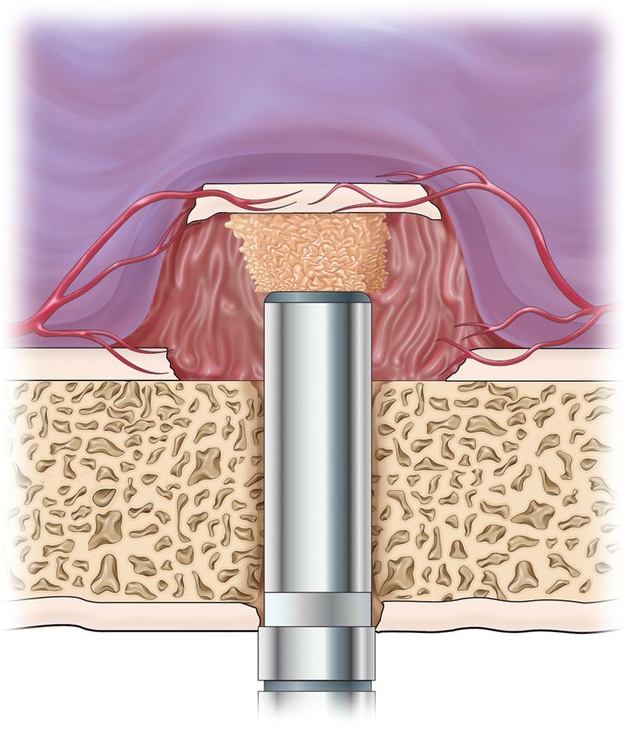
Fig 15-6a The use of a 2-mm drill, stopped short of the sinus floor, allows accurate insertion of the osteotome. Vascularity of sinus membrane supplied by the superior alveolar, greater palatine, and infraorbital arteries.
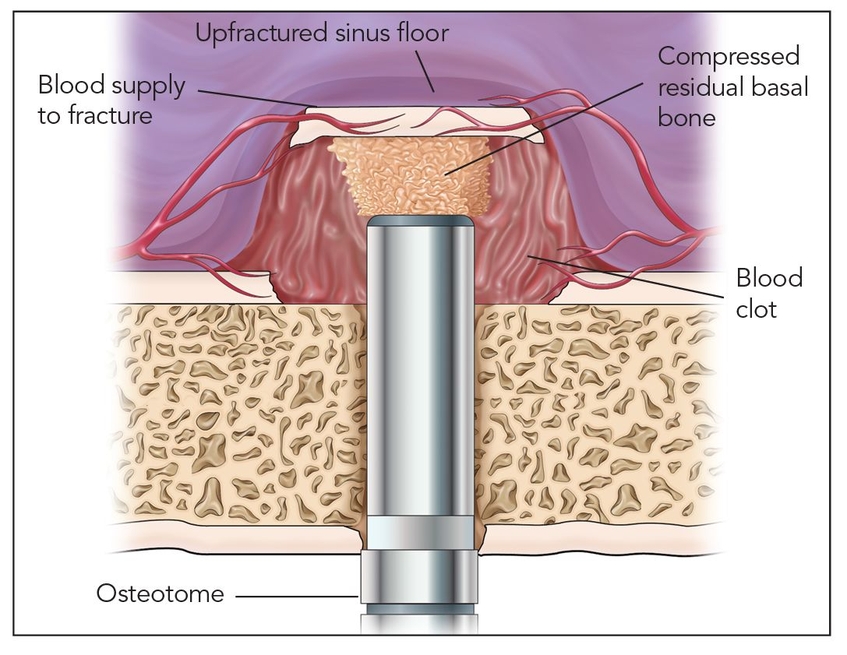
Fig 15-6b The osteotome compresses the remaining bone and fractures the sinus floor segment of bone that is larger than the diameter of the osteotomy is elevated.
Fig 15-6c When elevations are modest, about 4 mm, the membrane remains attached to the elevated sinus floor, and perforations are less likely. Membrane perforation and bone resorption of the graft are more common with elevations of 5 mm or greater.
/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


