Enamel
Learning Objectives
• Define and pronounce the key terms in this chapter.
• Describe the properties of enamel.
• Discuss the apposition and maturation of enamel.
New Key Terms
Abfraction (ab-frak-shen)
Abrasion (uh-brey-zhun)
Attrition (ah-trish-un)
Enamel (ih-nam-l) caries, dysplasia (dis-play-ze-ah), lamellae (lah-mel-ay), rod, spindles, tufts
Erosion (e-ro-zhun)
Imbrication lines (im-bri-kay-shun)
Interprismatic region (in-ter-priz-mat-ik)
Lines of Retzius (ret-zee-us)
Neonatal line (ne-oh-nate-l)
Perikymata (per-ee-ki-maht-ah)
Pit and groove patterns
Enamel
Preservation of the enamel of every tooth during a patient’s lifetime is one of the goals of every dental professional. Dental professionals must take into consideration the histology of enamel, as well as the properties of enamel, when deciding the caries risk for patients, counseling patients and communities on fluoride use, applying enamel sealants, and using and recommending polishing or toothpaste agents (discussed later).
Mature Enamel
Mature enamel is a crystalline material that is the hardest mineralized tissue in the human body (see Table 6-2). Enamel can endure crushing pressure of around 100,000 pounds per square inch; a layering of the deeper dentin and surrounding periodontium, coupled with the hardness of the enamel, produces a cushioning effect of the tooth’s differing structures enabling it to endure the pressures of mastication.
In its mature state, it is noted for its almost total absence of the softer organic matrix. Enamel in a healthy state, precluding trauma or disease, can be removed only by rotary cutting instruments or rough files such as those used in dental practice. Enamel is avascular and has no nerve supply within it. Although enamel is the hardest mineralized tissue in the body, it can be lost forever because it is nonvital and therefore not a renewable resource. However, it is not a static tissue, because it can undergo mineralization changes (discussed later).
Thus, mature enamel is by weight 96% inorganic material (or mineralized) 1% organic material, and 3% water. This crystalline formation of mature enamel consists of mainly calcium hydroxyapatite with the chemical formula of Ca10(PO4)6(OH)2. The calcium hydroxyapatite is similar to that found in lesser percentages in dentin, cementum, and alveolar bone. On radiographs, the differences in the mineralization of different parts of the tooth and surrounding periodontium can be noted. Enamel appears more radiopaque (or lighter) than either dentin or pulp because it is denser than the latter structures, both of which appear more radiolucent (or darker).
Other minerals, such as carbonate, magnesium, potassium, sodium, and fluoride, are also present in smaller amounts. Studies have challenged this composition of enamel, and, instead, maintain that it is mainly carbonated hydroxyapatite because of its relationship with fluoride uptake. Whatever the true formation, the crystals of enamel are set at different angles throughout the crown area. Discussion of the elegant crystalline nature of enamel is awkward at best, but this chapter is an attempt to do justice to this beautiful, jewel-like material.
Enamel is usually the only part of a tooth that is seen clinically in a healthy oral cavity because it covers the anatomical crown (see Figure 15-8). Enamel provides a hard surface for mastication and speech; it is able to withstand the masticatory impact of 20 to 30 pounds of pressure per tooth. It shows a thin layer in the cervical areas and is thicker in masticatory areas, such as at the incisal edges and cusps, where impact can be greater.
Enamel also provides the pleasing whiteness of a healthy smile. Enamel alone is various shades of bluish white, which is seen on the incisal ridge of newly erupted incisors, but it turns various shades of yellow-white elsewhere because of the underlying dentin (see Figure 6-18). The enamel on primary teeth has a more opaque crystalline form, and thus appears whiter than on permanent teeth.
Because the overall shade of enamel varies in each person and possibly within a dentition, a shade value is taken when integrating tooth-colored
 Clinical Considerations about Enamel Pathology
Clinical Considerations about Enamel Pathology
One way that enamel and other hard tissue of the tooth are lost is through attrition, which is the wearing away of hard tissue as a result of tooth-to-tooth contact (Table 12-1). Tooth wear from attrition increases with age. Permanent first molars wear more than seconds; seconds more than thirds. Attrition is discussed in Chapter 20 with regard to parafunctional habits (see also Figures 16-8, 16-17, 16-25, 20-8). The relationship between the loss of the vertical dimension of the face and alveolar bone loss is discussed in Chapter 14. Enamel loss may also result from friction caused by excessive toothbrushing and abrasive toothpaste. This wear is considered abrasion.
TABLE 12-1
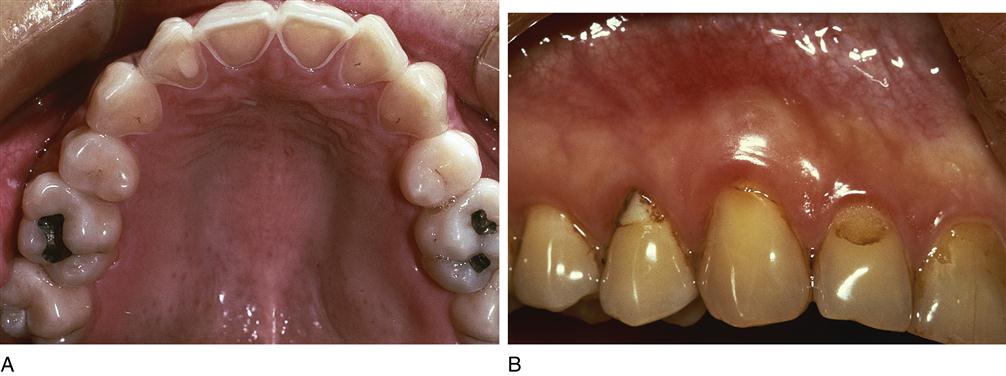
Enamel can also be lost by erosion through chemical means. Erosion is particularly apparent in patients with the eating disorder of bulimia, in which patients force themselves to vomit to remove their stomach contents in pursuit of weight loss (Figure 12-1). The lingual surface of the anterior teeth and the occlusal surface of all the teeth are eroded by the acid content of the vomit. The yellow underlying dentin is thereby exposed and can undergo attrition, because it is less mineralized than enamel. Treatment of bulimia is multifactorial and includes behavior changes. Similar erosion can be caused by gastric reflux, as well as certain recreational drug use (“meth mouth”). If facial enamel lesions of the anterior teeth are evident, the patient may be overusing acid-containing carbonated soft drinks and sport or health drinks (especially diet formulations and those containing enamel-eroding citric acid).
Another way that enamel and other hard tissue of the tooth can be lost is by enamel caries. Caries is a process through which a cavity is created by demineralization, or loss of minerals. This demineralization is due to acid production by cariogenic bacteria (discussed later) and occurs to enamel when the pH is less than 5.5 (see later discussion).
Finally, enamel can be lost as a result of abfraction (see Figure 12-1, B). Abfraction is thought to be caused by tensile and compressive forces during tooth flexure, which possibly occurs during parafunctional habits with their occlusal loading (see Chapter 20). It consists of cervical lesions that cannot be attributed to any particular cause, such as erosion or toothbrush abrasion; abfraction causes the enamel to pop off, starting at the cervical region, thus exposing the area to possible further wear, dentinal hypersensitivity, or caries.
restorative materials or artificial teeth or crowns within an individual dentition. The goal is to match, as closely as possible, the color of the patient’s other teeth. This shade value is selected by comparing the patient’s natural teeth to a shade guide of plastic model crowns that have been moistened and are viewed in natural light. These shade guides are provided by various manufacturers. New technology allows a digital read-out of the color of the enamel (whitening process is discussed later.)
Apposition of Enamel Matrix
Amelogenesis is the process of enamel matrix formation that occurs during the stage of app/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


