Dental Implants
Chapter Objectives
On completion of this chapter, the student will be able to:
1. Describe the basic types of implants used in dentistry today.
2. Describe the different types of metals used for dental implants.
3. Explain osseointegration of an implant.
4. Discuss the clinical care of dental implant fixtures.
6. List the home care aids for implants and explain how they are used.
KEY TERMS defined with the chapter
Subperiosteal Implant implant placed on top of the bone and under the periosteum
Transosteal Implant implant that penetrates entirely through the bone
Endosseous (Endosteal) Implant implant placed into the bone
Alloy a mixture of two or more metals
Osseointegration bone growing into intimate contact with an implant
Implant fixture metal cylinder placed into bone to support a crown or prosthesis
Implant abutment metal component that connects the implant crown to the implant fixture
Healing abutment replaces the cover screw when the top of the implant fixture is uncovered and it allows soft tissue to adapt to it
Impression abutment used in the implant impression to align the implant analog in the same way as the fixture was in the mouth
Implant analog a replica of the implant fixture that is used in the laboratory fabrication of the implant crown
Historically and currently, the most widely used material in restorative and corrective dentistry is metal. Use of metal dental implants has been growing rapidly. This chapter discusses the types of implants with emphasis on endosseous implants because they are the most widely used. Their placement, integration with bone, components, and maintenance are discussed. It is essential that the dental hygienist have an understanding of the characteristics of the various metal materials to correctly manipulate and care for them. The dental assistant and hygienist must be able to answer questions by patients relative to the material and techniques that will be used for their treatment.
Implant Materials
Implant metals have been used in orthopedic medicine for many years and more recently in dentistry. Dental implants are used as anchors for prosthetic replacement of missing teeth. Their use is expanding as implant materials and techniques continue to improve, and their success rate remains high (90% or more) with careful case selection. Implants can be used to replace one or more single units as individual crowns or as fixed bridges, or they can support a partial or full denture. In the mandible, atrophy (loss through resorption of the bone) of the alveolar ridge is common in patients who have lost teeth at a relatively young age. A complete denture often has very little retention in this circumstance. Implants can help to retain and stabilize the denture. Implants are of three main types: subperiosteal, transosteal, and endosseous (Figure 11-1). Endosseous implants are the most commonly used in dentistry today.
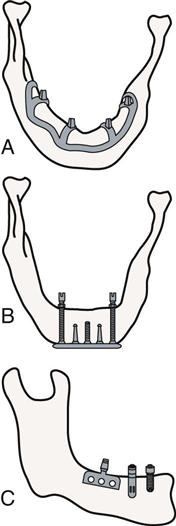
Subperiosteal Implants
Subperiosteal implants are placed under the periosteum (a fibrous covering of the bone) and rest on the bone. They are constructed and placed in three stages. First, a surgical incision is made to expose the bony ridge by reflecting the soft tissue and periosteum overlying the bone. An impression is made of the exposed bone. The surgical wound is closed. Second, a replica is made of the bony ridge from the impression. A metal framework is cast in the laboratory to fit over the bone. It has metal projections on which the prosthesis will be attached that extend through the tissues covering the ridge. Third, a second incision is made to reopen the initial wound and once again expose the bone. The implant framework is inserted over the bone and under the periosteum. The overlying tissues are sutured closed with the metal projections for the prosthesis protruding into the oral cavity. This type of implant is most commonly used in the mandible. It is rarely used in present-day dentistry and has been replaced by endosseous implants.
Transosteal Implants
The transosteal implant (also called a mandibular staple) is used to support a mandibular denture when the patient has severe resorption and lacks enough bone support for endosseous or subperiosteal implants. It consists of a horizontal support beam attached to metal rods that are inserted into holes drilled all the way through the mandible from its superior border to the inferior border. A metal plate through which the ends of the rods pass is bolted to the underside of the mandible. A transosteal implant requires both intraoral and extraoral incisions for its placement and stabilization. It is seldom used because of its highly invasive nature.
Endosseous Implants
Endosseous (endosteal) implants are surgically placed into the bone. These are the most popular implants currently in use and will be the focus of the implant discussion. Clinical studies have shown these implants to be very successful with long-term survival (greater than 10 years) of approximately 85% in the maxilla and 95% in the mandible. The difference in success rates between the two jaws is related to the quality of the bone in each jaw. The bone in the mandible is generally much denser. Over the years, a variety of endosseous implant designs and materials have been used. Today these implants are typically cylinders of various configurations depending on the manufacturer and may include surface irregularities, screw-like threads, or a hollow core with or without holes through its sides. The expectation is that these surface designs will help the integration of the bone with the implant.
Titanium and titanium alloys are the metals most commonly used because of their favorable biocompatibility with the oral tissues. Titanium is a lightweight, corrosion-resistant material. Bone will grow around and fuse to titanium implants (a process called osseointegration) intimately enough to retain them. Pure titanium is not as rigid or strong as titanium alloy, and this property can occasionally lead to failure of the implant if it is placed under heavy loading forces (such as with patients who grind their teeth a lot). Pure titanium quickly forms a thin surface layer of oxides that will integrate with the bone. Titanium alloys contain small amounts of vanadium and aluminum to improve their physical properties, particularly their strength. A thin surface coating of calcium phosphate (in the form of hydroxyapatite) or plasma proteins is added by some manufacturers to the titanium fixture to enhance osseointegration.
Other materials that have been used for dental implant fixtures are ceramics, composites, vitreous carbon, and polymers. These materials have been used with limited success. Negative aspects of the ceramic type are its brittleness and lack of flexibility, thus it can transmit greater stress to the implant site and itself is a poor material for withstanding functional forces. Composite and polymer implant fixtures did not integrate with the bone.
Endosseous Implant Placement and Restoration
Variations are seen in the surgical approaches to implant placement and in healing times before the crown or other prosthesis is placed. Part of the decision depends on whether there is already a healed edentulous space or whether a tooth needs to be extracted first.
Two-Stage Surgical Procedures
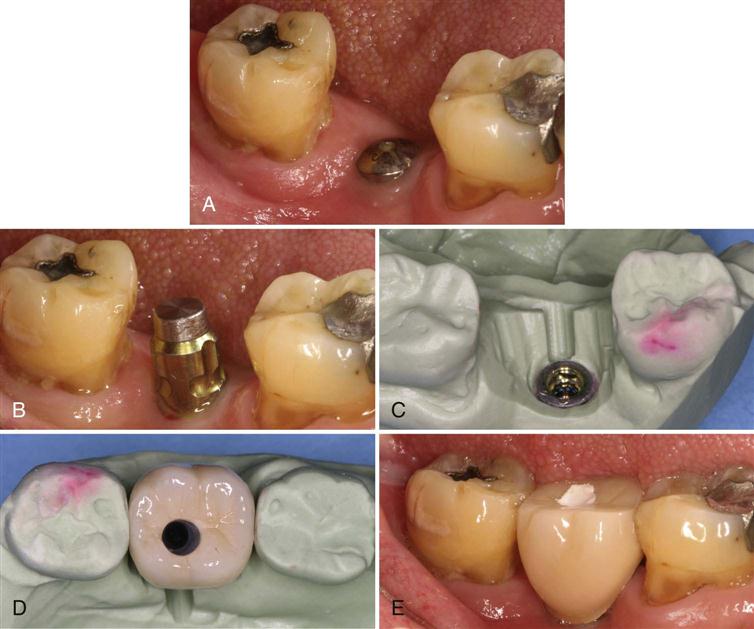
The surgical procedures are done in two stages. When an implant is placed in two stages, the first stage involves exposing the bone at the chosen placement site with a surgical flap. Next, a hole is drilled in the bone that is the shape and length of the implant cylinder and a size that is just slightly smaller than the cylinder. Depending on the implant fixture design, the implant is either lightly tapped into place to have a frictional fit with the bone, or it is screwed into place. Often an acrylic resin surgical guide (called a stent) is made ahead of time with holes drilled through it at the same angulation at which the implant should be positioned. The surgeon places it over the ridge at the time of surgery and inserts a bone-cutting bur through the predetermined holes to cut the hole for the implant at the correct angulation. The stent is particularly helpful when the surgeon has to place several implants that need to be parallel to each other for purposes of the restoration that will be placed on the implants. It is important that excessive heat not be generated during drilling of the bone. The bone can be damaged easily and then will not integrate with the implant cylinder (also called a fixture). After the implant fixture is placed in the bone, a screw is placed into the opening at the top of the fixture. The surgical flap is repositioned and sutured closed over the implant. Approximately 3 months later, the surgeon uncovers the top of the implant fixture, removes the screw, and places a smooth dome-shaped component called a healing abutment (Figure 11-2, A) that screws onto the top of the fixture. Next, the soft tissue (gingiva) is positioned around the healing abutment, leaving it exposed to the oral cavity while the gingiva heals around it. This process allows the gingiva to form a border or cuff around the implant, which will adapt to the crown when it is placed. After a few weeks, the crown impression procedure can begin.
One-Stage Surgical Procedure
With the one-stage procedure, surgery for placement of the implant is performed just as with the two-stage procedur/>
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


