Chapter 10
Hard Tissue Surgery (Ridge Augmentation) for Dental Implants
Aim
The aim of this chapter is to outline the role of bone augmentation procedures in relation to dental implant placement.
Outcome
Having read this chapter the reader will be aware of the need for implant placement to be planned from a restorative perspective and when surgical bone augmentation may be utilised to provide predictable results.
Introduction
Traditionally the site of dental implant placement was determined by the location of available bone, and this frequently resulted in sub-optimal implant positioning. Implant treatment planning should be carefully integrated into a holistic restorative plan in order to obtain an acceptable final result. Thought should therefore be given at the initial planning stage to both the prosthetic and the surgical aspects of implant therapy. Surgeons have traditionally either relied on basic surgical stents or placed implants by free hand; however, both methods make it difficult to visualise the final restorative result. Optimal implant position and angulation are crucial to successful restoration, and errors of as little as 1 mm in position or 5° in angulation can significantly and adversely affect the final restoration.
It is common for patients to present for implant reconstruction several years after the loss of their dentition, and the resultant alveolar bone loss presents a major problem for fixture placement. Similarly, the progression of periodontal disease and traumatic injury may result in both tooth loss and loss of supporting hard and soft tissues. When the quantity and quality of bone is inadequate, bone augmentation procedures facilitate reconstruction of the alveolar ridge, allowing for optimal placement and anchorage of implant fixtures.
Various systems have been employed over the years to classify the deficient alveolar ridge, including that of Lekholm and Zarb (1985), Cawood and Howell (1998) and Palacci and Ericsson (2001). The management of deficient alveolar ridges particularly in the anterior maxilla presents a challenge to the surgeon and prosthodontist.
A variety of bone-grafting materials have been advocated and the evidence base for success at five years appears to be satisfactory. The “gold standard” material for bone grafting remains the autogenous bone graft, although the use of allogenic and alloplastic materials is still cited in the literature (Chapter 5).
Autogenous bone grafts can be harvested from several sites (Table 10-1). The major advantages of such grafts appear to be their high osteogenic and osteoinductive potential and rapid conversion to vital bone. Autogenous bone grafts are applied using either an onlay or inlay technique, using either block (Figs 10-1 and 10-2) or particulate grafting techniques. One of the potential problems, as outlined at the planning stage, is that when there is inadequate bone there is often inadequate soft tissue, in terms of both quantity and quality, to cover the graft. This frequently necessitates the need for peri-implant soft tissue augmentation procedures (Chapter 11). However, soft tissue surgery is not a substitute for inadequate hard tissue management around dental implants (Chapter 11).
| Extra-oral sites | Intra-oral sites |
| Iliac crest (Fig 10-10) | Chin |
| Calvaria | Lateral ramus of mandible |
| Coronoid process | |
| Maxillary tuberosity |
Fig 10-1 Block graft from chin (Courtesy of Palacci, Esthetic Dentistry).
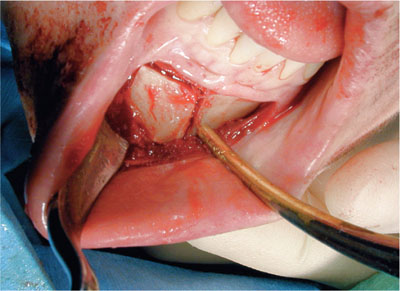
Fig 10-2 Block graft from chin being harvested.
Operative Management
Bone Augmentation Procedures for the Anterior Maxilla
Bone augmentation of the anterior maxilla is complicated by the requirement for both aesthetics and function in this area. Although particulate grafts can sometimes be used, in conjunction or not with rigid or resorbable membranes, this provides generally less predictable outcomes compared with the use of cortico-cancellous block grafts (Fig 10-3). The graft of choice in this region is often dependent on the volume of bone required; the more bone necessary, the greater the need for block grafting. Anterior maxillary grafting often necessitates the use of both horizontal and, occasionally, vertical augmentation procedures.
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


