Introduction
In this study, we aimed to determine the effect of bone mineral density (BMD), cortical bone thickness (CBT), screw position, and screw design on the stability of miniscrews.
Methods
Ninety-six miniscrews of both cylindrical and tapered types were placed in 6 beagle dogs. The BMD and CBT were measured by computerized tomography and correlated with the placement and removal torque and mobility. A regression equation to predict the placement torque was calculated based on BMD, CBT, screw type, and screw position.
Results
The placement torque showed a positive correlation in the order of removal torque (0.66), BMD of the cortical bone (0.58), and CBT (0.48). Placement and removal torque values were significantly higher in the mandible compared with the maxilla. Tapered miniscrews had higher placement torque than did the cylindrical type ( P <0.001). However, the removal torque was similar in both groups. Placement torque was affected by screw position, screw type, and BMD of cortical bone, in that order.
Conclusions
BMD of cortical bone, screw type, and screw position significantly influence the primary stability of miniscrews.
Easy placement is an advantage of orthodontic miniscrews. In addition, the tooth can be moved without the patient’s cooperation; this enhances treatment efficiency. Some success has been reported regarding the use of miniscrews as orthodontic anchorages. However, the clinical application of a miniscrew does not guarantee treatment success, and its stability is essential before it can be used as orthodontic anchorage.
It is important to ensure the initial stability of an orthodontic miniscrew because most failures occur during the initial stage. Furthermore, stability of the miniscrew in the initial stage reduces its micromovement, thus allowing for an appropriate environment that supports the healing process surrounding the bone. The success of an implant or miniscrew is determined by the patient’s general condition, the biocompatibility of the materials, the placement procedure, and bone quantity and quality. The initial stability of miniscrews is considered essential in clinical use because of immediate or early loading in many patients.
Two factors affect the initial stability of a screw: the screw factor and the host factor. The screw factor is related to the characteristics of the screw design, including diameter and length. Various screw designs have been introduced to enhance initial stability. The goal is to increase initial fixation by inducing controlled compressive forces in the cortical bone layer. In the prosthodontic field, it was reported that a tapered shape can enhance stability for immediate loading by increasing the mechanical contact between the dental implant and the surrounding bone.
The host factor is related to the quantity and quality of the bone where the screw is placed. Cortical bone thickness (CBT) (quantity) can affect the initial stability of a screw. Finite element analysis showed that, when a lateral force is applied to the screw, most of the force is concentrated on the cortical bone. For this reason, the previous studies focused on the anatomic background related to CBT rather than bone quality, to improve the stability of the miniscrew.
On the other hand, several studies have used computed tomography (CT) in prosthodontics and orthopedics to study factors related to bone density. It was reported that bone density differs according to sex, age, and physical condition. CT was recently suggested to successfully measure bone mineral density (BMD) in orthopedics. BMD has been used as a parameter to establish a treatment plan to ensure the stability of implants in dentistry.
There are 2 methods for measuring BMD. One is with Hounsfield units (HU), and the other is to measure BMD indirectly by using a hydroxyapatite block. Since Hounsfield units can be affected by the loaded voltage of x-rays and the protocol used, bone density analysis with a BMD calibration standard (hydroxyapatite block) has greater advantages for evaluating bone quality more accurately.
One assessment method of initial stability is to measure the torque during placement. Cheng et al proposed that placement torque could be used as an indicator for initial stability, and, to obtain initial stability, a certain amount of torque is necessary. Placement torque is the measurement of the resistance at the screw-bone interface; it reflects the level of bone deformational strain caused by the miniscrew.
In this study, we hypothesized that BMD values can be used to predict the mechanical stability of miniscrews by evaluating placement torque. Our aim was to determine the effect of BMD, CBT, screw position, and screw design on the stability of miniscrews.
Material and methods
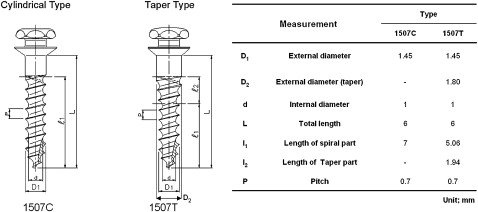
For this study, miniscrews were placed in 6 beagle dogs (age, 1 year; weight, 12 kg). Their purchase, selection, and management, and the experimental procedures were carried out according to prescribed conditions of the institutional review board, the Animal Experiment Committee of Yonsei Hospital, Seoul, Korea. A nondrilling type of miniscrew, 1.4 mm in diameter and 7 mm in length, was used. Both the cylindrical type (OAS-1507C) and tapered type (OAS-1507 T, Biomaterials Korea, Seoul, Korea) were selected; 96 screws were used ( Fig 1 ).
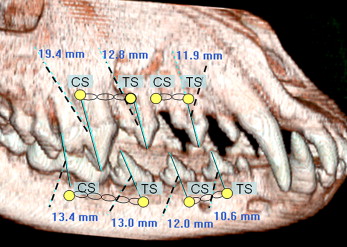
The location of the orthodontic miniscrew placement was determined after evaluating the reconstructed CT image, taken before placement, to determine whether there was sufficient interdental space. Sites selected were between the roots of the second, third, and fourth premolars, and the first molar in the mandible, between the roots of the second and third premolars, the first molar, and between the second and third premolars in the maxilla ( Fig 2 ).
The animals were injected subcutaneously with 0.05 mg per kilogram of atropine followed by an intravenous injection of rompun, 2 mg per kilogram, and ketamine, 10 mg per kilogram, to induce general anesthesia. The anesthesia was maintained with 2% enflurane, and each animal’s temperature was maintained with a heating pad and an electrocardiogram, and monitored. When placing the mini-implant, 2% hydrochloric acid lidocaine containing 1:100,000 epinephrine was infiltrated into the placement area. Before placement, a 5-to-10 mm gingival incision was made under saline-solution irrigation, and complete placement of the screw into the alveolar bone was confirmed.
Screw placement was performed manually with 70° to 90° angulations to gingival surface in consideration of the buccolingual width of alveolar bone for each experiment. In all miniscrews, a force of 250 to 300 g was applied with an elastomeric chain engaged reciprocally from a cylindrical miniscrew to a tapered miniscrew immediately after the placement of miniscrews, and the elastic chain was exchanged every 3 weeks.
Screw mobility was measured twice on each miniscrew by using a periotest (Simens AG, Bensheim, Germany) before removing the screw. The sleeve of the handpiece of the periotest was positioned with 1 to 2 mm from the screw head perpendicularly after an elastomeric chain was removed. The average of 2 measurements for a miniscrew was recorded as the mobility value. During the test period, a chlorhexidine solution was applied daily to maintain the animals’ oral hygiene ( Fig 3 ).
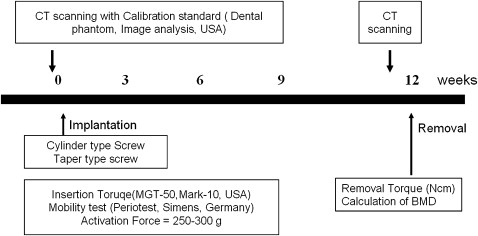
The placement torque was the highest (in newtons per square centimeter) when the miniscrew was placed completely into the bone. The highest removal torque was measured during a quarter initial turn by using a torque sensor (MGT50, Mark-10 Co, New York, NY).
To measure the BMD of the implanted area, CT scanning was done 3 days before placing and removing the miniscrews. Before scanning, each dog was placed under intramuscular sedation. The gantry of the CT device was placed parallel to the occlusal plane, and the dog’s head was fixed with a strap. The CT scan was performed with a high-speed advantage CT scanner (GE Medical System, Milwaukee, Wis) by using standard CT protocol (high-resolution algorithm, 512 × 512 matrix, 120 Kv, 200 mA) at a table feed of 6 mm per second. The CT data were reconstructed to 1-mm thick transaxial images.
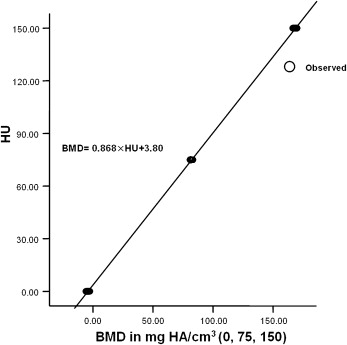
A calibration standard (Dental Phantom, Image Analysis, Columbia, Ky) was applied to calibrate the level in Hounsfield units in the dogs during the CT scanning. The calibration standard containing 3 compartments with 0, 75, and 150 mg of hydroxyapatite per cubic centimeter was attached to the phantom for BMD calibration. Calibration was performed by measuring the Hounsfield unit values in the 3 compartments of the dental phantom and relating these values to determine the BMD with a linear equation. The calibrations were performed for each dog.
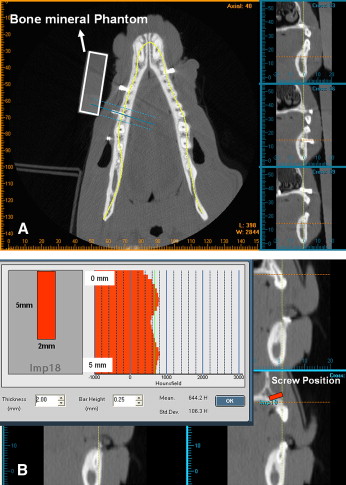
The scanned images were analyzed by V-implant (CyberMed, Seoul, Korea). The CT data taken before removing the screws were reconstructed to a transaxial image at 1-mm intervals for each occlusal plane of the maxilla and mandible ( Fig 4 , A ). The vertical location and inclination of each screw was localized by using a reconstructed image at the coronal plane from the postoperative scans. This information was transferred to the preoperative images. From the preoperative scanning data, the average BMD of a cylindrical area (diameter, 2 mm; depth, 5 mm) for each screw site was measured as the BMD total by Hounsfield unit calibration. The CBT and average bone mineral density in the cortical area (BMD cortical) were also calculated ( Fig 4 , B ).
Statistical analysis
To determine the relationship between Hounsfield units and BMD values, a calibration regression equation was derived individually for all experimental dogs and was based on a linear relationship: BMD = a HU + b, where a and b are calibration coefficients.
Pearson correlation analysis was used to determine the association between placement torque, removal torque, mobility, BMD, and CBT. The categorical variables (screw type and position) were statistically evaluated by using independent t tests to determine any differences in placement torque. The results suggest that the variables were linearly correlated. Thus, a multiple regression model was used with placement torque as the dependent variable, and CBT, BMD, screw type, and screw position as the independent variables.
Results
A regression equation was obtained by using the average Hounsfield value ( Table I , Fig 5 ) for the 3 parts in the standard calibration of each beagle. The parameter a (inclination) was calculated within the range of 0.813 to 0.935, and the intercept b ranged from 3.80 to 24.47. The correlation coefficient of all regression equations was >0.98.
| Dog | Calcium hydroxyapatite | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 mg/cm 3 | 75 mg/cm 3 | 150 mg/cm 3 | |||||||
| HU | HU | HU | Calibration coefficients | ||||||
| Mean | SD | Mean | SD | Mean | SD | Parameter a | Parameter b | Correlation coefficient | |
| 1 | −4.2 | 0.8 | 81.6 | 0.7 | 168.7 | 1.1 | 0.868 | 3.80 | 0.99 |
| 2 | −6.4 | 6.2 | 79.4 | 2.6 | 176.9 | 6.3 | 0.813 | 7.24 | 0.99 |
| 3 | −3.9 | 1.8 | 82.3 | 3.0 | 178.8 | 3.4 | 0.819 | 4.76 | 0.99 |
| 4 | −10.8 | 5.3 | 74.1 | 2.1 | 169.8 | 4.0 | 0.827 | 10.71 | 0.99 |
| 5 | −7.6 | 2.0 | 53.0 | 4.9 | 149.8 | 1.4 | 0.935 | 14.16 | 0.99 |
| 6 | −21.0 | 5.7 | 47.8 | 2.3 | 160.4 | 1.4 | 0.810 | 24.47 | 0.98 |
A correlation was observed between placement and removal torque, mobility, screw type, and BMD cortical. The mobility showed a negative correlation with placement torque (–0.577) and a positive correlation with BMD cortical (0.575) ( Table II ).
| Variable | Correlation coefficient | P value |
|---|---|---|
| Removal torque | .661 | 0.001 |
| Mobility | −.577 | 0.001 |
| CBT | .476 | 0.001 |
| BMD cortical | .575 | 0.001 |
| BMD total | .078 | 0.504 |
Stay updated, free dental videos. Join our Telegram channel
VIDEdental - Online dental courses


